
Articles
- Page Path
- HOME > J Korean Acad Community Health Nurs > Volume 33(1); 2022 > Article
- Original Article The Effect of Depression on Quality of Life in Patients with Parkinson's Disease: Mediating Effect of Family Function
- Eun Sook Bae, Hye Seung Kang
-
DOI: https://doi.org/10.12799/jkachn.2022.33.1.105
Published online: March 31, 2022

2Assistant Professor, Department of Nursing, Saekyung University, Yeongwol, Korea
- 895 Views
- 43 Download
- 1 Crossref
- 0 Scopus
Abstract
Purpose
The purpose of this study is to explore the roles and function of family in mediating the relationship between depression and quality of life of patients with Parkinson’s disease (PD). Most studies have found that depression is particularly common in patients with PD and further associated with poor quality of life. Family function, as a mediator, is based on a strength orientation perspective that emphasizes not only their responsibilities and risks but also recuperative powers and growth potential.
Methods
Overall 157 adults with idiopathic Parkinson’s disease were enrolled in this study via outpatient clinic and completed a set of assessment to measure depression using BDI, family APGAR questionnaire, and patients’ quality of life using PDQ-8. Hierarchical multiple regression analysis was conducted to examine the mediating role of family APGAR score in the relationship between BDI and PDQ-8.
Results
Patients' depression, gait disturbance, duration of illness, and family function were statistically significant on quality of life. These factors accounted for 60% of the variance in quality of life. Family function has a partial mediating effect on the relationship between depression and quality of life.
Conclusion
Findings from the study suggest that although PD patients' depression impacts their quality of life, by having strong family function, the extent to which depression impacts the quality of life can be favorably mitigated. Additionally, these outcomes have important implications for future model development regarding PD patients.
| J Korean Acad Community Health Nurs. 2022 Mar;33(1):105-113. English. Published online Mar 31, 2022. https://doi.org/10.12799/jkachn.2022.33.1.105 | |
| © 2022 Korean Academy of Community Health Nursing | |
Eun Sook Bae ,1
and Hye Seung Kang2 ,1
and Hye Seung Kang2
| |
|
1APN, Gerontological Nursing, Suyeong Hyodo Hospital, Busan, Korea. | |
|
2Assistant Professor, Department of Nursing, Saekyung University, Yeongwol, Korea. | |
Corresponding author: Kang Hye-Seung. Department of Nursing, Saekyung University, 197, Hasong-ro, Yeongwol-eup, Yeongwol 26239, Korea. Tel: +82-33-371-3164, Fax: +82-33-371-3239, | |
| Received August 22, 2021; Revised February 21, 2022; Accepted February 22, 2022. | |
|
This is an Open Access article distributed under the terms of the Creative Commons Attribution Non-Commercial License (http://creativecommons.org/licenses/by- | |
|
Abstract
| |
|
Purpose
The purpose of this study is to explore the roles and function of family in mediating the relationship between depression and quality of life of patients with Parkinson’s disease (PD). Most studies have found that depression is particularly common in patients with PD and further associated with poor quality of life. Family function, as a mediator, is based on a strength orientation perspective that emphasizes not only their responsibilities and risks but also recuperative powers and growth potential.
Methods
Overall 157 adults with idiopathic Parkinson’s disease were enrolled in this study via outpatient clinic and completed a set of assessment to measure depression using BDI, family APGAR questionnaire, and patients’ quality of life using PDQ-8. Hierarchical multiple regression analysis was conducted to examine the mediating role of family APGAR score in the relationship between BDI and PDQ-8.
Results
Patients' depression, gait disturbance, duration of illness, and family function were statistically significant on quality of life. These factors accounted for 60% of the variance in quality of life. Family function has a partial mediating effect on the relationship between depression and quality of life.
Conclusion
Findings from the study suggest that although PD patients' depression impacts their quality of life, by having strong family function, the extent to which depression impacts the quality of life can be favorably mitigated. Additionally, these outcomes have important implications for future model development regarding PD patients. |
|
Keywords:
Parkinson disease; Quality of life; Depression; Family
|
|
|
INTRODUCTION
|
Parkinson’s Disease (PD) is major geriatric neurodegenerative diseases, along with dementia and stroke, and its incidence rate is increasing worldwide as being an aging society [1]. According to data from the National Health Insurance Review and Assessment Service (NHISS) [2], the number of PD patients has increased from 71,571 in 2010 to 125,927 in 2020, an increase of 1.8%. Based on statistics for 2020, PD patients aged 70 years or older account for more than 83.5% of Parkinsonian syndrome cases. Also, 31.6% of male, 68.4% of female showed that female Parkinson's patients were twice as likely as male Parkinson's patients. The cost of PD treatment has increased from 384 billion won in 2016 to 483 billion won in 2020, a steady increase of 6% annually. Parkinson's patients’ costs are around 2 times higher than non-Parkinson's patients.
PD is a progressive neurodegenerative disease that leads to various motor and cognitive dysfunction. It is a serious disease accompanied by both physical and mental damaging effects on patients [3]. The dysfunction is accompanied by both physically and cognitive symptoms due to damages in neurons. Motor symptoms include tremors, rigidity, bradykinesia, and unstable posture. These symptoms result in limited self-care function, then often cause depression in PD patients [4]. Research has been conducted in other countries for the past 20 years to improve the quality of life of PD patients, but South Korea has been conducting research for the last ten years. The patients’ quality of life, cognitive function, and depression have been studied mostly in the fields of medicine, rehabilitation, and nursing, while quality of diet, well-being, and effects of exercise have been studied in the fields of nutrition and exercise [5].
Depression the most common non-motor symptom, is prevalent among adult neurological patients and occurs in 30~50% of patients with PD [6]. Depression occurs early phase of PD and negatively affects daily life performance and quality of life in patients suffering from PD [7]. Depression commonly occurs in the early stage of PD, and it not only affects physical disability, cognitive deterioration, and the quality of daily living, but it can also result in the misdiagnosis of either apathy or amnestic disorder related to dementia as depression with PD [5]. Therefore, depression management in PD patients improves individual well-being and becomes an evaluation index that indicates health status or therapeutic efficacy [6]. Since only the patient's symptoms are controlled and maintained among various therapeutic methods including pharmacological and non-pharmacological interventions, such as music therapy [8] are beneficial for depression in PD patients.
As the chronic illness progresses, the family must assume important responsibilities such as coping with their emotional state, role changes, efficient problem solving, and utilization of external resources [8]. Family function reflects the family's ability to satisfy the needs of the family members in terms of communication and sharing among the family members, and it is closely associated with the individual's health and illness [9]. It has been reported that the burden of care under long-term care, expectations when preparing to cope with the risk of fatigue, and family dysfunction negatively affect the physical and psychological state, and even the general well-being of the family caregivers [10]. It is necessary to enhance family function to improve the quality of life for PD patients [11]. Family functions were positively related to quality of life of caregivers of PD patients [12].
It is known that patients with serious symptoms of depression usually have low family function and have difficulty in normal life [13, 14]. Cancer patients who complain of severe symptoms of depression tend to come from broken homes and have poor quality of life when compared to patients with low levels of depressive symptoms or receiving palliative care [13]. Patients with type 2 diabetes show that depressive symptoms are related to family dysfunction and impaired quality of life. That is, depression was negatively related to family function and family function had a good influence on better quality of life in patients [14].
Previous studies have shown connections among patients’ depression, family function, and quality of life [13, 14]. There is research on the relationship between depression and quality of life [5, 7, 8] and is research on the relationship between family function and quality of life [11, 12]. Based on the finding that patients’ quality of life is closely related to psychological and family functioning factors, a relationship can be established among the three variables. Until now, the relationships among the three variables have not been identified for PD patients, thus it is the need to verify direct and indirect effects. This study aimed to examine the relationship among depression, family function, quality of life and validate the mediating effect of family function between depression and quality of life. This study is expected to showcase strategies to improve quality of life for PD patients.
|
METHODS
|
1. Study Design
This is a cross-sectional descriptive study that aimed to investigate the effects of depression on quality of life of PD patients and the mediating effects of family function.
2. Setting and Sample
Data were collected from outpatients with PD at hospital in B metropolitan city. The selected patients had been diagnosed with PD according to the standards of the Korean Parkinson disease Association and were being treated as outpatients. Those who have been diagnosed with PD for more than six months and belonged to one of the Hoehn and Yahr stages 1~3 (Stage 4, which is a severely disabled state, and stage 5, which is a bedridden state if no help or wheelchair is provided, were not included). They were able to communicate and had Mini-Mental State Examination (MMSE) scores of 24 or higher (no cognitive impairment). Exclusion criteria were: (a) current drug abuse, (b) psychosis or bipolar disorder, and (c) severe depression defined as over 30 on Montgomery Asberg Depression Rating Scale-Self rating version, MADRS-S. Gait disturbance is recognized as one of the core diagnostic criteria and may present as short, shuffling steps, gait freezing, lurching unsteady gait, or spontaneous falls [15] and was measured in terms of no sign (0 point) or signs over once per month (1 point).
Sample size based on G*Power 3.1.9 program [16] estimates were calculated. The minimum number of sample total 136 participants were estimated to be required for performing multiple regression analysis, with eight predictors, an effect size of 0.15, a significance level of α=.05, and a statistical power of 0.90. The effect size was based on previous research on depression and quality of life in Parkinson's patients [17]. Considering the calculated result of 136 participants and a 20% dropout rate, a total of 170 questionnaires were distributed. However, 13 were excluded from the analysis due to the survey was not completed or questions were omitted, and data of 157 outpatients were analysed.
3. Measurements
1) Depression
The presence and severity of depressive disorder was assessed using the Beck depression inventory (BDI) [18]. The instrument used in the present study utilized the Korean version translated by Lee [19]. Depression is an emotional disorder ranging from mood swings to pathological states such as anxiety, gloom, helplessness, and worthlessness, and to measure depression, The BDI consists of 21 items covering emotional and physiological symptoms. The Cronbach’s α of Beck [18]’s study was .85 and Cronbach’s α of Lee [19]’s study was .98. In the present study, the Cronbach’s α was .93
2) Family function
For assessing family function, the Korean version of family APGAR (Adaptability, Partnership, Growth, Affection, and Resolve) questionnaire originally developed by Smilkstein et al. [20] and translated by Kang et al. [21] was used. The following five factors were utilized for family function: adaptability, partnership, growth, affection, and resolve. In the family The Cronbach’s α of Smilkstein et al. [20]’s study was .80. ln the present study, the Cronbach’s α was .89.
3) Parkinson’s disease quality of life
A shortened form of the Parkinson’s Disease Questionnaire (PDQ-8) devised by Jenkinson et al. [22] was used; one item was selected from each of the eight areas of mobility, activities of daily living, emotional well-being, stigma, social support, cognitions, communications, and bodily discomfort of the Long-form 39-item (PDQ-39) version [23]. PDQ-8 is measured on a 5-point scale, with a possible score range of 8 to 40, and higher scores indicating better quality of life. The scale was translated in Korean by this researcher and was approved for use by the original developer via mail. After translation, two nursing professors evaluated and revised the PDQ-8 Korean version. The present investigator obtained similar results to that of the PDQ-39 [23] in terms of validity and reliability, and PDQ-8 [22] also reported Cronbach’s α in the range of .73 to .88 in their study across five countries (Canada, Italy, Spain, USA, and Japan). In a study conducted by the developers of the Korean version [8], Cronbach’s α was .72. In the current study, the Cronbach’s α coefficient was .84.
4. Data Analysis
Statistical Package for Social Sciences (SPSS) software (version 20, Korea) was used for all analyses. Descriptive statistics were used to compare demographic variables, depression, family function, and quality of life score. Cronbach's α values were measured to ensure the reliability of the instruments. Differences between groups were analyzed using the non-parametric test when normality test are not satisfied. Difference tests analysis was performed using the Kruskal-Wallis H test, and a post hoc analysis was performed using the Bonferroni-Dunn.
The mediating effects of family function on depression and quality of life were analyzed using Baron and Kenny's three-step test procedure for mediating effects [24], which employs simple and multiple regression analyses. Perfect mediation holds if the independent variable has no effect when the mediator is controlled. Partial mediation holds if the independent variable has an effect when the mediator is controlled.
5. Ethical Consideration
The Institutional Review Board of Dong-A University approved this study (IRB No.17-045). To ensure the practicality of the questionnaires, two professors participated in training sessions to formulate the reliability of the measures. Therefore, all participants could understand the question items and it took them approximately 30 minutes to complete the tests. Participants were required to complete the demographic surveys, and measures of depression, Family Functioning, and Quality of life according to their actual feelings. Responders who were too ill to reply to questions or who were illiterate dictated their responses and their replies were recorded. The collected data were then checked for completeness. All subjects volunteered to participate and gave their written informed consent after receiving an explanation of the study. Subjects’ anonymity was preserved, and there was no penalty for withdrawing from the study, which they could do at any time.
|
RESULTS
|
1. Characteristics of the Study Participants
Patients’ sociodemographic are shown in Table 1. Patient ages ranged from 53 to 90 years, with a mean of 68.01 years, 45.9% were male, and 54.1% were female. 85.5% patients were married. A total of 30.8% had a high school education. Average age of onset was 61.95 years. An illness duration of <1~3 years was the most common (27.6%), and 26.9% had a duration of 9 years. A total of 45.9% patients had gait disturbance.
|

The analysis of depression showed median (interquartile range) scores of 22 (12~36), and mean scores of 8.41 and 31.71 points for family function and quality of life, respectively (Table 1).
2. Differences in Depression, Family function, and Quality of Life according to Sociodemographic Characteristics
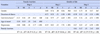
Table 2 provides the results of the analysis of the differences in depression, family function, and quality of life according to sociodemographic characteristics. The depression score was statistically higher for female than male (t=19.78, p=.039), and showed statistically higher score of patients with gait disturbance (t=17.60, p=.005). The family function score showed statistically higher for patients with over 75 years than patients with 55~59 years (H=13.01, p=.023), and showed statistically lower score of patients with gait disturbance than those who didn’t gait disturbance (t=25.54, p=.038). Quality of life score was statistically higher for male than female (t=29.50, p=.026), and showed statistically lower score of patients with gait disturbance than those who didn’t gait disturbance (t=14.82, p<.001).
|

3. Correlations among Depression, Family Function, and Quality of Life of Patients with PD
The quality of life of patients was deeply interconnected with depression (r=-.67, p<.001) and family function (r=.42, p<.001). It was adversely associated with depression but positively associated with family function. The depression was significantly negatively correlated with family function (r=-.38, p<.001) (Table 3).
|

4. Hierarchical Multiple Regression Analysis of Quality of Life
We determined that patients’ depression and quality of life were strongly related to family function by using hierarchical regression multiple analysis. The control variables were as follows: age of onset and gait disturbance, which showed significant differences in family function in the mean difference test; gender; duration of illness; and gait disturbance, which showed significant differences in quality of life.
In the first step depression has a significant negative effect on family function (β=-.31, p<.001). That is, family function decreases as depression increases. The control variable that significantly influenced the mediating variable family function was found to be age of onset (β=.35, p=.010), which indicates that as the age of onset increases, family function decreases; however, gait disturbance was not significant.
In the second step depression had a significant negative influence on quality of life (β=-.52, p<.001). That is, quality of life decreased as depression increased. In this case, the control variables that significantly influenced quality of life, were duration of illness (β=-.21, p<.001) and gait disturbance (β=-.27, p<.001). which indicate that the quality of life decreased when the patient's duration of illness increased, and when the patient suffered from gait disturbance. The explanatory power of the independent variable on the dependent variable was 58%.
In the third step, both the independent and mediating variables were entered simultaneously. The test results of the influence of the independent variable depression and the mediating variable family function on the dependent variable quality of life carried out showed that the influence of both depression (β=-.47, p<.001) and family function (β=.15, p=.020) were significant. Family function was found to have a partial mediating effect between depression and quality of life since the regression coefficient (β=-.47) of depression was smaller in the third step than the regression coefficient (β=-.52) of depression in the second step [23]. In this case, the control variables that had a significant influence on the dependent variable quality of life were duration of illness (β=-.20, p<.001) and gait disturbance (β=-.26, p<.001), which indicates that quality of life improved when the duration of illness decreased and when the patient did not suffer from gait disturbance. The model fit of regression analysis was significant (F=27.59, p<.001), and the explanatory power of the independent variables on the final dependent variable was 60%(Table 4).
|
5. Mediating Effect
The results of the Sobel test [25] additionally conducted to find out if the mediating effect of family function was significant in the relationship between depressive state and quality of life showed |Z|<1.96, which indicates that family function served an intermediary role since the mediating effect of family function was statistically significant at the level of 0.05 (Table 4, Figure 1).
|

|
DISCUSSION
|
Results of this study found that 77% of PD patients suffer from the symptoms of depression, with an average score of 23.37 points, indicating moderate depression. These findings were like more than 70% of the depressive prediction model studies in Parkinson's patients who showed these depressive symptoms [26]. There is a high risk for the progression of depression as the negative impact of depressive symptoms is more prominent relative to the symptoms of PD itself.
First, the present study found that depression in PD patients affects family function. In addition, the fact that the age of onset was found to be a factor affecting family function is the cause of family dysfunction because the sudden onset of illness brings on problems not only in the role of the head of household and supporting the family but also economic problems and psychological stress. The findings of the present and previous studies share common ground in that when PD patients suffer from high levels of depression, their family function and quality of life tend to be low. Previous cancer studies [13] have reported prevalence rates of 32% for depression and family function problems in 50% of cancer patients receiving palliative care.
PD is a progressive disease so a patient’s condition can worsen gradually. In that case, the patient’s family members must deal with constant pain, need to adapt to a whole new set of responsibilities, and care for the patient, which is very taxing and exhausting. In addition to the increasing physical hardship, financial burden, and little hope of complete recovery, families confront ever increasing suffering [9]. The adjustment process, such as the family caregiver adjusting to the care situation, developing appropriate coping strategies, and adjusting to changes in emotional and social support brings about changes in the functioning of the family [12].
Secondly, patients with low depressive symptoms showed high levels of family function and quality of life. The findings of the current study agree with the findings of a previous study, which depression affecting quality of life of the elderly in PD [27]. In addition, the showed that depression strongly impacts quality of life of PD patients [28]. Since depression due to PD affects physical disability, cognitive decline, and the difficulty of daily living [6], it can be understood that Gait disturbance and difficulty in daily activities can affect quality of life. It was found that depression had substantial negative association with impaired quality of life and low levels of depression can lead to better quality of life.
Thirdly, the analysis results showed a partial mediating effect of family function in that the explanatory power of depression directly influencing quality of life was 58%, whereas the explanatory power of depression influencing quality of life with family function acting as a mediating variable was 60%. The results showed that when depression of patients with PD worsens, the patient will have greater disability than patients without depression, and patient's depression directly influencing the quality of life. In this case, strengthening family function can ultimately improve the quality of life of the patient since it reduces the caregiving burden so that based on a positive relationship with the patient. Available methods of utilizing family members include family participation in nursing care planning, and organization of a self-help group communication program.
Similar findings were seen in a study of type 2 diabetic patients. There were links between depression, family function, and quality of life. When family function of type 2 diabetic patients was low, the quality of life was low and when the patient suffered from depression, impaired family function was evident [14]. Such a result indicates the necessity of education that increases bonding among family members and adaptability by having the family members participate when conducting an intervention for PD patients.
As a chronic degenerative disease progresses for an extended period, a fundamental measure of long-term patient care rather than a temporary one should be proposed [9]. The symptoms that change with the progression of disease bring unexpected stresses to the patient and the family since they frequently occur suddenly, and communication within the family can be affected not only by the illness but also by a series of psychological responses and coping strategies [12]. Conducting family therapy and counselling, for patients suffering from Parkinson’s disease and depression is recommended to improve family function so that patients with depression can find a new path to share their feelings with significant family members or to strengthen the family bonding and adaptability, or to educate the caregivers about the disease.
Finally, the present study investigated relationships among depression, family function, and quality of life of PD patients and the results showed that depression was associated with family dysfunction and impaired quality of life [13, 14]. Family function as a mediator contributed to depression and it in return contributed independently towards various dimensions of quality of life. When one of the most challenging issues for a family is how to maintain a functionally balanced mutual relationship, they often experience a profound crisis when new relationships must be figured out, and where the possibilities for closeness are often very different, limited, and skewed [21]. This study implies that family function is beneficial when they can cope with problems arising from an illness or disability in ways that are empowering, sustain hope, and affirm their relationships. By providing family function assessments, family therapy, and family interventions [10, 11, 12], nursing service can provide a way to reduce depressive symptoms and enhance the quality of life of patients with PD.
Furthermore, the program to improve quality of life for patients with PD should be designed to develop nursing strategy for social participation and use the community resources [27]. According to data from the NHISS [2], PD patients' economic activity population (40~50s) rate is 9 times higher than dementia. therefore, program to overcome Parkinson's disease by utilizing community resources is required. At the overseas research, an integrated, multidisciplinary care setup involving different healthcare professionals is the mainstay in the management of PD [29]. In Singapore, nurse-led integrated community care program for PD to provide care in community and at patient’s home [30]. In United Kingdom., Parkinson's disease specialist nurse system is being introduced and to reduce hospitalization and outpatient costs to less than 50%. The Netherlands is introducing an advanced system that applies multidisciplinary approach. PD is a complex syndrome of numerous symptoms and mechanisms, because management of it can be managed by a teamwork of various groups of experts to increase efficiency [30]. Therefore, a special interest by the government in PD is needed in both the medical and community.
The present study looked at the association of depression, family function, and quality of life in PD patients, and found that depression has been shown to affect quality of life through family function. However, a limitation of this study was that it was conducted with 157 PD patients who visited only one hospital, thus making it difficult to generalize the results to all patients with the disease. PD is a chronic, progressive neurodegenerative disease, so more cohort studies are needed to establish protective or preventive therapies through follow-up. Another limitation of this study is a lack of specific history regarding the treatments (including drugs and other diseases) for the PD patients.
|
CONCLUSION
|
This study is meaningful in that it conducted a study on clinical patients with PD and confirmed the family function as a factor influencing the quality of life. To improve the efficiency of nursing interventions for PD patients, measures that ultimately enhance the quality of life of patients by improving their adaptability through the evaluation of family function, as well as continuous provision of social and emotional support should be investigated. Since the current research was implemented on PD patients in a local area, caution should be taken in interpreting the results. Future research is recommended comparatively analyses the interceding effect of family function on PD patients with depression. That should be encouraged to reduce depression and improve quality of life by providing family communication, family therapy, and education as interventions to increase family function.
|
References
|
 Cite
Cite
