Articles
- Page Path
- HOME > Res Community Public Health Nurs > Volume 34(3); 2023 > Article
-
Original Article
- Factors Affecting the Performance of Infection Control of Multi-drug Resistant Organisms in Intensive Care Unit Nurses of General Hospitals based on the Theory of Planned Behavior: The Mediating Effect of Intention
-
Nam-Sook Kim1
 , So-Eun Choi2
, So-Eun Choi2 -
Research in Community and Public Health Nursing 2023;34(3):183-195.
DOI: https://doi.org/10.12799/rcphn.2023.00150
Published online: September 27, 2023
1Team Manager, Infection Control Office, Mokpo Christian Hospital, Jeollanam-do, Korea
2Professor, Department of Nursing, Mokpo National University, Jeollanam-do, Korea
- Corresponding author: Choi So-Eun Department of Nursing, Mokpo National University, 1666 Yeongsan-ro, Chenggye-myeon, Muan-gun, Jeollanam-do, 58554, Korea Tel : +82-61-450-2672 FAX : +82-61-450-2679 E-mail : seami@mnu.ac.kr
Copyright © 2023 Korean Academy of Community Health Nursing
This is an Open Access article distributed under the terms of the Creative Commons Attribution NoDerivs License. (http://creativecommons.org/licenses/by-nd/4.0) which allows readers to disseminate and reuse the article, as well as share and reuse the scientific material. It does not permit the creation of derivative works without specific permission.
- 1,242 Views
- 85 Download
Abstract
-
Purpose
- The purpose of this study is to analyze the factors that affect the performance of infection control of multidrug-resistant organisms (MDROs) by nurses in intensive care units (ICU) in general hospitals.
-
Methods
- Participants were 105 ICU nurses from 6 general hospitals. The questions for the survey performed were based on the theory of planned behavior, such as attitude towards infection control of MDROs, subjective norms, perceived behavioral control, intention, and performance.
-
Results
- In the relationship between subjective norms towards infection control of MDROs and performance, intention showed a significant complete mediating effect; and in the relationship between perceived behavioral control and performance, intention showed a partial mediating effect. The attitude towards infection control of MDROs was excluded from the mediating effect verification because there was no significant correlation between intention and performance.
-
Conclusion
- The results of this study suggest that department atmosphere and perceived behavior control promotion programs should be developed to enhance subjective norms in order to promote the performance of infection control of MDROs.
- 1. Background
- The development of antibiotics has been used as an innovative method to treat bacterial infections, but the misuse and overuse of antibiotics have led to the emergence of multi-drug resistant organisms (MDROs) [1]. MDROs are defined as microorganisms that are resistant to one or more classes of antimicrobial agents [2], and MDRO infections are reported to increase the economic burden due to prolonged hospital stay and the incurrence of additional medical costs, and show high morbidity and mortality rates [3,4]. Various intervention strategies for infection control of MDROs can decrease medical costs of individual patients, and reduce the increase of national healthcare expenditure at a national level [3]. Therefore, in the U.S., the Centers for Disease Control and Prevention (CDC) has been implementing systematic infection control against MDROs through standardized, evidence-based clinical practice guidelines, including accurate diagnosis and treatment, a judicious use of antibiotics, and compliance with standard precautions and contact precautions to prevent the transmission of MDRO infections [2]. In Korea, a sentinel surveillance system for healthcare-associated infectious diseases has been established and operated for 6 types of MDROs [5]. Also, Methicillin–resistant Staphylococcus aureus (MRSA), Vancomycin–resistant Enterococci (VRE), multi–drug resistant Acinetobacter baumannii (MRAB), and multi-drug resistant Pseudomonas aeruginosa (MRPA) have been designated as Group 4 infectious diseases, and a sentinel surveillance system for them has been implemented [5]. These policy changes regarding infection control reflect the increasing seriousness of MDORs in healthcare settings [6]. MDORs can be spread within medical institutions mainly through direct and indirect contact with patients or medical devices, and in particular, there is an increasing risk of infection through invasive medical devices [7]. Especially, patients in intensive care units (ICUs) have difficulty maintaining skin integrity due to the application of invasive medical devices such as peripheral and central venous catheters, and they are at increased risk for infection because the use of immunosuppressants and underlying diseases such as diabetes can compromise host defense mechanisms against infection [8]. In a study on the comparison between antibiotic resistance rates of isolated strains from ICU patients and non-ICU patients, the antibiotic resistance rates of MRSA strains from ICU patients and non-ICU patients were 84% and 58%, respectively, and the antibiotic resistance rates of VRE strains from ICU patients and non-ICU patients were 34% and 19%, respectively, revealing that isolates from ICU patients showed higher antibiotic resistance rates [9]
- MDRO infections may be transmitted to other patients through medical personnel who have frequent contact with patients [2], and among medical staff members of medical institutions, nurses have many opportunities to come into contact with patients since they provide patients with various non-invasive or invasive nursing activities, so nurses have a very important role in the implementation of infection control in healthcare settings [10]. In studies on the actual status of infection control of MDROs, a larger size of medical institutions and greater availability of manpower and other resources for infection control were found to be associated with a stricter implementation of infection control against MDROs [11]. In addition, general hospitals were shown to have a lack of resources for infection control in overall areas, including manpower, a system, and facilities for infection control [12]. In addition, the percentage of hospitals with the ICU equipped with isolation rooms for isolation treatment of patients infected with MDROs was found to be 100% for tertiary hospitals and 86.6% for general hospitals [13]. As described above, since general hospitals are more likely to experience a lack of resource support for infection control against MDROs compared to tertiary general hospitals, ICU nurses of general hospitals are expected to have greater difficulty in carrying out infection control against MDROs than ICU nurses of tertiary general hospitals.
- Regarding previous studies on infection control against MDROs among ICU nurses in Korea, prior studies on infection control among ICU nurses of tertiary general hospitals examined perception of infection control [14] or investigated the knowledge and practice of inflection control [15-17]. Meanwhile, in prior studies on infection control among ICU nurses of general hospitals, the knowledge and practice of inflection control [18] and infection control against VRE [19] were investigated. In these studies, the method of infection control education, satisfaction with infection control education, perception of empowerment and environmental safety [18], age, education level, and isolation environment [15] were identified as factors affecting the performance of infection control against MDROs among ICU nurses, and research was mostly focused on analysis of relationships between variables or the investigation of influencing factors. As described above, since a number of previous studies in Korea were conducted without applying a conceptual framework or a theory, they had limitations in systematically investigating factors affecting the practice of infection control of MDROs and relative effects of influencing factors. Therefore, this study intends to apply the theory of planned behavior (TPB) proposed by Ajzen [20], since the TPB is generally regarded as an excellent theory for predicting the behaviors of individuals. According to the TPB, since intention is a motivation factor for performing a behavior, stronger intention is associated with a higher likelihood of performing the behavior, and intention is influenced by three variables: attitude toward the behavior, subjective norm, and perceived behavioral control. In other words, the TPB claims that ‘attitude’ toward the behavior, ‘subjective norm’, which is related to other people’s opinions or perceptions, and ‘perceived behavior control’, which is related to one’s perception of factors hindering the behavior, influence a particular behavior through intention acting as a mediating variable [20].
- With respect to previous studies on infection control applying the TPB, a prior research reported that attitude, subjective norm, and perceived behavioral control were found to be predictors for behavioral intention, and that perceived behavioral control was identified as a direct predictor for performance [22]. In addition, some previous studies found that perceived behavioral control, subjective norm, and intention had a direct effect on performance, while attitude was not an influencing factor for performance [17,23]. Meanwhile, some research found that intention had a direct effect on performance, but perceived behavioral control did not have any effect on it [21]. As described above, the findings of previous studies applying the TPB are partially inconsistent in terms of the explanatory power of measured variables and relationships between variables, depending on study participants and the type of behavior studied. However, the results of prior studies applying the TPB suggest that intention is a strong influencing factor for behavior. Therefore, noting the importance of the role of ICU nurses in the implementation of infection control to prevent MDRO infections in patients in the ICU, in order to improve the performance of infection control against MDROs in ICU nurses, this study aimed to identify factors affecting the performance of infection control against MDROs based on the TPB through the verification of the mediating effect of intention among major variables of the TPB. Through this investigation, the present study purported to provide basic data for the development of intervention strategies to enhance the performance of infection control against MDROs among ICU nurses of general hospitals.
- 2. Objectives
- Based on the theory of planned behavior (TPB), this study aimed to identify factors influencing the performance of infection control against MDROs in ICU nurses of general hospitals through the verification of the mediating effect of intention, an antecedent factor of behavior, among major variables of the TPB. The specific objectives of this study are as follows:
- 1) To examine differences in attitude, subjective norm, perceived behavioral control, intention, and performance regarding infection control of MDROs according to the characteristics of participants:
- a. To examine attitude, subjective norms, perceived behavioral control, intention, and performance regarding infection control of MDROs;
- b. To investigate correlations between attitude, subjective norm, and perceived behavioral control, intention, and performance regarding infection control of MDROs;
- 2) To investigate the mediating effect of intention in the relationships between attitude, subjective norm, perceived behavioral control, and performance regarding infection control of MDROs.
Introduction
- 1. Study design
- This study is a descriptive survey research based on the theory of planned behavior, and this research aimed to identify factors affecting the performance of infection control of MDROs among ICU nurses of general hospitals, and investigate the mediating effect of intention, an antecedent variable of behavior, among major variables from the theory of planned behavior.
- 2. Participants
- The participants of this study were nurses working in intensive care units (ICUs) of 6 general hospitals located in J Province, and they were selected by convenience sampling. The sample size was calculated using the G-power 3.1 program. The effect size was determined using an explanatory power of 23.4%, based on a previous study by Gu et al. [17], which reported that the explanatory power of factors influencing the performance of MDRO infection control guidelines was 23.4%. The minimum sample size for multiple regress analysis was determined to be 96 persons with a significance level of .05, a power of 0.80, and 19 predictor variables. The 19 predictor variables included 14 general characteristics as well as variables from the theory of planned behavior, such as attitude, subjective norms, perceived behavioral control, and intention. Taking into account the dropout rate of 10% and the return rate of questionnaires, questionnaires were distributed to 110 persons, and a total of 110 copies were collected. Among them, a total of 105 copies were finally used in data analysis, excluding 5 respondents due to insincere responses. Regarding the inclusion criteria, participants were selected among nurses with at least 3 months of experience in working as an ICU nurse, and only persons who understood the purpose of the study, and provided written informed consent to participate were included in this study. Nursing managers of ICUs who did not directly participate in the care of ICU patients and newly employed nurses were excluded from this study.
- 3. Measures
- Attitude toward infection control of MDROs was measured using the assessment tool presented by Gu et al. [17] after obtaining approval for its use from the authors. Gu et al. [17] created an assessment tool for attitude toward performance of MDRO infection control guidelines by modifying an instrument developed by Moon & Song [23]. The original instrument proposed by Moon & Song [23] was intended to assess attitude toward the performance of healthcare-associated infection control guidelines. The scale for attitude toward infection control of MDROs used in this study is composed of 5 items. Each item was rated on a 7-point Likert scale ranging from 1 point (Strongly disagree) to 7 points (Strongly agree). Higher scores indicate more positive attitude toward the performance of MDRO infection control guidelines. Regarding the reliability of the scale, the value of Cronbach α was .75 in the study by Gu et al. [17], and it was .80 in this study.
- Subjective norm about infection control of MDROs was assessed using the assessment tool proposed by Gu et al. [17] after obtaining approval for its use. Gu et al. [17] devised a measurement tool for subjective norm about performance of MDRO infection control guidelines by modifying a tool developed by Moon & Song [23]. The original scale created by Moon & Song [23] is an instrument designed to measure subjective norm about the performance of healthcare-associated infection control guidelines. The assessment tool used in this study consists of 2 items. Each item was rated on a 7-point Likert scale ranging from 1 point (Strongly disagree) to 7 points (Strongly agree). Higher scores indicate higher pressure from people around the individual about the performance of infection control against MDROs. Regarding the reliability for the assessment scale, the value of Cronbach α was .78 in Gu et al. [17] and it was .66 in this study.
- Perceived behavioral control about infection control of MDROs was measured with the tool presented by Gu et al. [17] after receiving approval for its use. Gu et al. [17] created an assessment tool for perceived behavioral control about the performance of MDRO infection control guidelines by revising a tool developed by Moon & Song [23], which was an assessment tool for perceived behavioral control about the performance of healthcare-associated infection control guidelines. The assessment tool for perceived behavioral control used in this study is composed of 5 negative questions. Each item was rated on a 7-point Likert scale ranging from 1 point (Strongly disagree) to 7 points (Strongly agree). All items were reverse scored, and higher scores indicate higher levels of the ability to control factors that impede the performance of infection control of MDROs. As to the reliability of the tool, the value of Cronbach α was .74, and it was .76 in the present study.
- Intention for infection control of MDROs was assessed using a tool presented by Gu et al. [17] after obtaining approval for its use. Gu et al. [17] created an assessment instrument for intention about the performance of MDRO infection control guidelines by revising a tool developed by Moon & Song [23]. The original scale developed by Moon & Song was an instrument designed to assess subjective norm about the performance of healthcare-associated infection control guidelines [23]. The assessment tool for intention of infection control of MDROs is composed of 3 items. Each item was rated on a 7-point Likert scale ranging from 1 point (Strongly disagree) to 7 points (Strongly agree). Higher scores indicate stronger intention to perform MDRO infection control guidelines. Regarding the reliability for the assessment tool, the value of Cronbach α was .77 in Gu et al. [17], and it was .84 in this study.
- The performance of infection control of MDROs was measured using a tool presented by Gu et al. [17] after obtaining approval for its use from the authors. Gu et al. [17] created an assessment tool for the performance of MDRO infection control guidelines by revising a tool developed by Shon & Park [15]. The original tool developed by Shon & Park [15] was an assessment scale for infection control performance of ICU nurses.
- The assessment scale for MDRO infection control performance used in this study is composed of a total of 22 items, which include questions about general infection control measures, such as sharing information about precautions, hand washing, wearing protective equipment, instrument management, and environment management, as well as questions about guidelines specific to each of the 6 types of MDROs. Respondents were asked to indicate their self-rated level of performance for each item. Each item was rated on a 5-point Likert scale ranging from 1 point (Hardly) to 5 points (Always). Higher total scores indicate higher levels of infection control performance of MDROs. Regarding the reliability for the assessment tool, the value of Cronbach α was .92 in both Gu et al. [17] and this study.
- 4. Data collection
- The participants of this study were nurses working in the ICUs of six general hospitals located in J Province. The researcher personally visited the ICUs of the six general hospitals over a period from November 15 to December 7, 2019, and obtained consent to participate from each hospital after explaining the purpose and methods of the study to the hospital director and nursing manager of each hospital. After explaining the purpose and procedures of the study to participants, a self-administered questionnaire survey was conducted only with persons who voluntarily agreed to participate and signed written informed consent. The completed questionnaires were collected by personal visit or by mail when it was difficult to collect questionnaires by personal visit.
- 5. Ethical Considerations
- To protect the rights of participants, this study was conducted after obtaining approval from the Institutional Review Board (IRB) of Mokpo National University after IRB review (Approval No.: MNUIRB-20190902-SB-006-01). Participants were given explanations about the purpose and methods of the study, and they were informed about their right to withdraw from this study at any time without any consequences if they wanted to. They were also informed that collected data would not be used for purposes other than research, and that all research data and records would be destroyed after storing them for 3 years from the date of study completion.
- 6. Statistical analysis
- The collected data was analyzed using SPSS/WIN 25.0, and specific analysis methods were as follows.
- Differences in the levels of attitude, subjective norm, perceived behavioral control, intention and performance regarding infection control of MDROs according to the characteristics of participants were examined using the t-test and one-way ANOVA. The levels of attitude, subjective norm, perceived behavioral control, intention and performance regarding infection control of MDROs were analyzed by calculating frequencies, percentages, means, and standard deviations. Also, Pearson's correlation coefficient was used to examine relationships between attitude, subjective norm, perceived behavioral control, intention, and performance regarding infection control of MDROs.
- In addition, the three-step mediated regression analysis proposed by Baron & Kenny [24] was used to examine the mediating effect of intention in the relationship of the performance of infection control of MDROs with attitude, subjective norm, and perceived behavioral control regarding infection control of MDROs. In the Baron and Kenny method of mediation analysis [24], the first step is regression analysis for the effect of independent variable on the mediating variable, the second step is regression analysis for the effect of the independent variable on the dependent variable, and the third step is regression analysis for the effects of the independent and mediating variables on the dependent variable. In the third step, both the independent and mediating variables are simultaneously entered into the regression model to conduct regression analysis after controlling for the effects of the variables on each other. To demonstrate that a variable has a significant mediation effect, it needs to be shown that the mediating variable has a significant effect in the first and second regression analyses, and additionally, the effect size for the effect of the independent variable on the dependent variable needs to be reduced in the third regression analysis compared to the effect size in the second regression analysis. At this time, if there is still a significant relationship between the independent and dependent variables, the mediating variable is considered to have a partial mediation effect, and if not, the mediating variable is considered to have a full mediation effect. The mediation test for the significance of the mediation effect was performed using the Sobel mediation formula (Z) [25]
Methods
1) Attitude toward infection control of MDROs
2) Subjective norm about infection control of MDROs
3) Perceived behavioral control about infection control of MDROs
4) Intention of infection control of MDROs
5) Performance of infection control of MDROs
- 1. Differences in attitude, subjective norm, perceived behavioral control, intention, and performance regarding infection control against MDROs according to the characteristics of participants
- The participants consisted of 86 females (81.9%) and 19 males (18.1%). In age, the 25-29 age group made up the largest proportion of participants at 45.7% (48 persons). As for education level, nurses with a bachelor’s or higher degree were 81 persons (77.1%), taking the largest proportion of participants, and nurses with an associate degree from three-year colleges made up 22.9% (24 persons). As to the length of clinical career, nurses with 1 to less than 5 years of clinical career made up the largest proportion of participants at 41% (43 persons). For the length of current position career, nurses with 1 to less than 3 years of career as an ICU nurse took the largest proportion of participants at 30.5% (32 persons). Regarding education on infection control against MDROs, 89 persons (84.8%) had the experience of receiving education on infection control against MDROs. In addition, both the rate of nurses with the experience of caring for patients with MDRO infections and the rate of hospitals with MDRO infection control guidelines were 100%. Regarding the level of satisfaction with MDRO infection control guidelines, 92 persons (87.6%) reported that they were satisfied with the guidelines. As a result of the analysis of differences in attitude, subjective norm, perceived behavioral control, intention, and performance regarding infection control against MDROs according to general characteristics of participants, it was found that there were no significant differences ( p>.05) (Table 1).
- 2. The levels of attitude, subjective norm, perceived behavioral control, intention, and performance regarding infection control of MDROs
- The mean scores for attitude, subjective norm, perceived behavioral control, intention, and performance regarding MDROs infection control were 5.97(±1.07) points, 6.51(±0.62) points, 5.61(±0.97) points, 5.74(±0.98) points, and 4.44(±0.46) points, respectively (Table 2).
- 3. Correlations between attitude, subjective norm, perceived behavioral control, intention, and performance regarding infection control of MDROs
- Infection control performance of MDROs showed a significant positive correlation with subjective norm (r=.24, p=.012), perceived behavioral control (r=.53, p<.001), and intention (r=.54, p<.001). Attitude toward infection control of MDROs was significantly positively correlated with subjective norm (r=.20, p=.038). Also, subjective norm about infection control of MDROs showed a significant positive correlation with perceived behavioral control (r=.35, p<.001), intention (r=.38, p<.001), and performance (r=.24, p=.012). In addition, perceived behavioral control about infection control of MDROs was found to have a significant positive correlation with intention (r=.67, p<.001) and performance (r=.53, p<.001). Furthermore, intention for infection control of MDROs had a positive correlation with infection control performance of MDROs (r=.54, p<.001) (Table 3).
- 4. The mediating effect of intention of infection control against MDROs
- To verify the mediating effect of intention for infection control of MDROs, a three-step mediation test was performed by the mediated regression analysis method proposed by Baron & Kenny (1986), and the results are shown in Table 4. Before performing regression analysis to verify the mediating effect, tests for multicollinearity, residuals, and outliers were performed to check assumptions for regression analysis. As a result, a correlation coefficient between independent variables of < .80, a tolerance of ≥0.55, a variance inflation factor (VIF) of ≤1.82, and a Durbin-Watson value of 1.69-1.93 were obtained, indicating that there was no multicollinearity or autocorrelation. In addition, to check the normality and homoscedasticity of the error term, the normal P-P plot and the scatter diagram were examined. As a result, all the variables were found to be normally distributed, and satisfaction of the homoscedasticity of individual residuals was also confirmed. Thus, regression analysis was carried out. Since there were no significant differences in variables related to infection control of MDROs according to general characteristics of participants (p >.05), the characteristics of participants were not included in regression analysis. In addition, since attitude toward infection control of MDROs was found to have no significant correlation with intention and performance (p >.05), it was also excluded from mediation analysis.
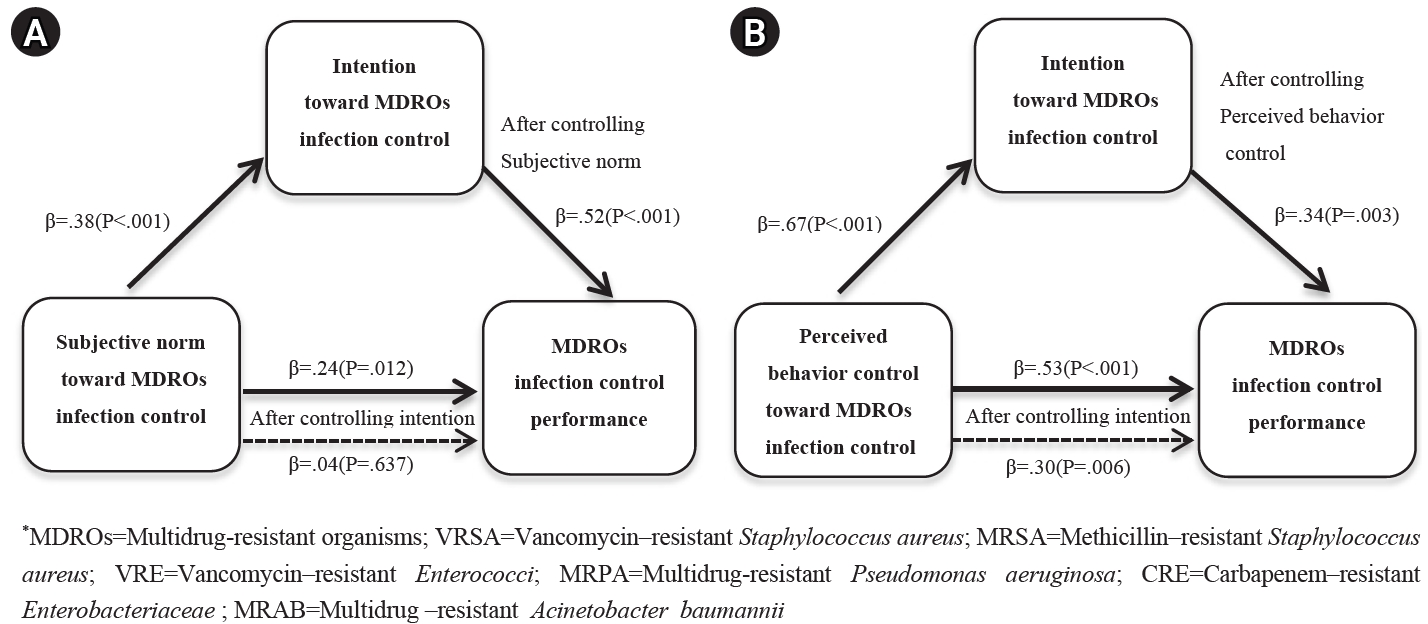
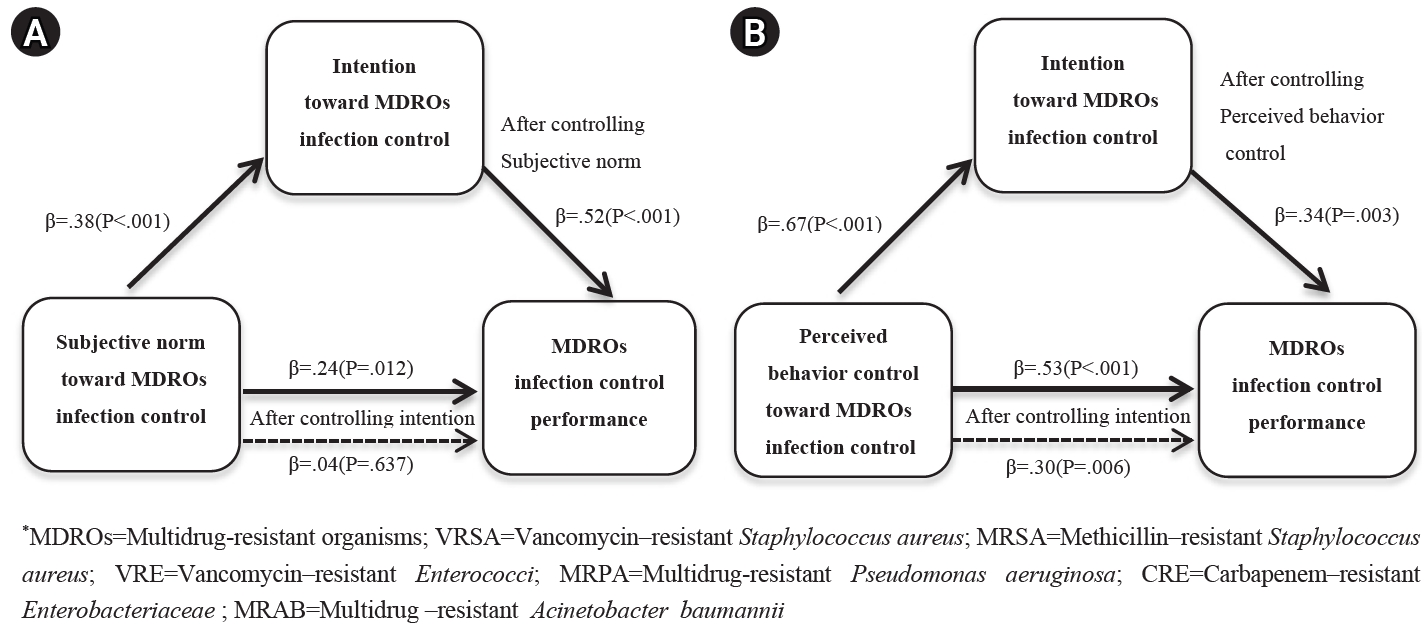
- To test the mediating effect of intention, regression analysis was performed by the method proposed by Baron & Kenny [24]. In the first step, subjective norm used as the independent variable was found to have a significant effect on intention, the mediating variable (β=.38, p<.001). In the second step, subjective norm used as the independent variable was found to have a significant effect on performance, the dependent variable (β=.24, p=.012). In the final third step, infection control performance of MDROs was entered as the dependent variable, and subjective norm as the independent variable and intention as the mediating variable were simultaneously entered into the regression model to conduct regression analysis after controlling for the effects of the variables on each other. As a result, it was found that intention had a significant effect on performance (β=.52, p <.001), but subjective norm did not have a significant effect on performance (β=.04, p =.637), indicating that intention showed a full mediation effect in the relationship between subjective norm and performance (Figure 1A). Additionally, the Sobel test was performed to test the significance of the mediating effect of intention for infection control of MDROs, and the results indicated that intention had a significant mediating effect in the relationship between subjective norm and performance (Z=3.57, p <.001) (Table 4).
- As a result of mediation analysis by the Baron and Kenny method [24], in the first step, perceived behavioral control used as the independent variable was found to have a significant effect on intention, the mediating variable (β=.67, p<.001). In the second step, perceived behavioral control used as the independent variable was found to have a significant effect on performance, the dependent variable (β=.53, p<.001). In the final third step, after MDRO infection control performance was entered as the dependent variable, perceived behavioral control as the independent variable and intention as the mediating variable were simultaneously entered into the regression model to conduct regression analysis after controlling for the effects of the variables on each other. As a result, both perceived behavioral control (β=.30, p=.006) and intention (β=.34, p=.003) were found to have a significant effect on intention. In other words, when intention was entered as a mediating variable, perceived behavioral control was shown to have a significant effect on performance, but the regression coefficient, which indicates the effect of the independent variable on the dependent variable, was decreased in the third step (β=.30), compared to the regression coefficient in the second step (β=.53), indicating that intention played a partial mediator role in the relationship between perceived behavioral control and performance (Figure 1B). Additionally, the Sobel test was conducted to determine the statistical significance of the mediating effect of intention about infection control of MDROs, and the results confirmed that the mediation effect of intention in the relationship between perceived behavioral control and performance was statistically significant (Z=3.04, p <.001) (Table 4).
Results
1) The mediating effect of intention in the relationship between subjective norm and performance
2) The mediating effect of intention in the relationship between perceived behavioral control and performance
- This study attempted to investigate factors affecting infection control performance of MDROs among ICU nurses in general hospitals, based on the theory of planned behavior (TPB), and verify the mediating effect of intention among major variables of the TPB, considering that intention is an antecedent factor of behavior.
- In this study, the levels of attitude (mean: 5.97 points), subjective norm (mean: 6.51 points), intention (mean: 5.74 points), and performance (mean: 4.44 points) regarding infection control of MDROs were similar to the results of a previous study of ICU nurses of tertiary general hospitals by Gu et al. [17] as well as the results of a prior study of nurses working in general wards by Moon & Song [23]. However, the mean score for perceived behavioral control (5.61 points) in this study is similar to 5.4 points reported by Gu et al. [17], but it was higher than 5.0 points reported by Moon & Song [23]. In this regard, considering that perceived behavioral control refers to the degree of ease and difficulty perceived by the individual in performing a particular behavior [20], the above-described difference or similarity in research results about perceived behavioral control is presumed to reflect the fact that ICU nurse with more experience in infection control of MDROs perceive that they are able to manage infection control, compared to general ward nurses. Although it was expected that there would be differences in infection control performance of MDROs in ICU nurses between general hospitals and tertiary hospitals as a result of differences in characteristics of general hospitals and tertiary hospitals, such as the characteristics and composition of medical personnel and hospital systems, the results of this study were similar to the findings of a previous study among ICU nurses in tertiary general hospitals [17]. In this connection, in Korea, the outbreak of Middle East respiratory syndrome (MERS) in hospitals and local communities in 2015 [26] increased social interest in infection control and raised questions about it, which led to the amendment of medical law related to infection control in October, 2016 [27]. As a result, the MERS outbreak and the consequential revision of medical law have brought about several changes in infection control policies, such as the introduction of infection control fees, establishment of standards of staffing and deployment of infection control manpower, and reinforcement of standards of infection control manpower by hospital size. A relatively higher score for perceived behavioral control in this study is presumed to reflect such infection control measures.
- Before examining the mediation effect of intention for infection control of MDROs, correlation analysis between variables was conducted. As a result, subjective norm, perceived behavioral control, and intention about infection control of MDROs were found to have a significant positive correlation with infection control performance of MDROs. In this regard, similar findings have been reported by a previous study on hand hygiene compliance in hospital nurses [21] and a prior study on the performance of MDRO infection control guidelines among ICU nurses [17]. As for attitude toward infection control of MDROs, although it was found to have a significant positive correlation with subjective norm, it did not show any correlations with infection control performance of MDROs. These results about attitude are similar to the findings of some previous studies. For example, a prior study reported that there was no significant relationship between attitude and performance regarding infection control of MDROs [17], and a previous study showed that there was no significant relationship between attitude toward hand hygiene and hand hygiene compliance [28]. However, some research reported that attitude toward hand hygiene was significantly positively correlated with the intention and compliance rate of hand hygiene [21]. These inconsistent study findings about attitude warrant replication research to elucidate the effect of attitude on performance.
- In this study, intention was found to have a full mediating effect in the relationship between subjective norm and performance regarding infection control of MDROs, and these results suggest that infection control performance can be improved through intention. Although there have been few similar studies to investigate the mediation effects of intention, the results of this study are consistent with the findings of some previous studies on intention of hand hygiene compliance. In particular, a study on intention of hand hygiene compliance reported that subject norm is an influencing factor for compliance intention [28], and another previous study found that intention of hand hygiene compliance has a direct effect on compliance behavior [21]. Subjective norm refers to the degree to which the individual perceives social pressure that requires him or her to perform infection control. Therefore, as a strategy to enhance subjective norms, it is recommended to create the atmosphere of the department through the leadership of superiors and positive feedback from colleagues. In this connection, a previous research about hand hygiene [29] studied the effectiveness of the implementation of protocol for hand hygiene. According to this previous study, the members of the infection control committee and department heads performed the role of a support group, and carried out activities such as hand hygiene education, promotion activities. Additionally, the study described that efforts to spread hand hygiene culture were made by methods such as vision presentation through leadership, promotional activities employing posters and screensavers, and education for all hospital personnel on how to properly wash hands. Regarding the effectiveness of the implementation of hand hygiene protocol, the study reported that it resulted in an increase in the hand hygiene compliance rate of overall hospital personnel and a year-on-year reduction in the incidence rate of MRSA bacteremia and the VRE detection rate during a study period [29]. According to Ajzen [20], intention is influenced by the three variables of attitude toward behavior, subjective norm, and perceived behavioral control, and stronger intention is associated with the higher likelihood of performing a particular behavior. In this study, intention was shown to have a full mediating effect in the relationship between subjective norm and performance regarding infection control of MDROs, and these results suggest that the enhancement of subjective norm and intention will lead to the improvement of infection control performance. Thus, in terms of strategies to improve infection control performance in ICU nurses, when the compliance rate of contact precautions, the hand hygiene performance rate, and the isolation rates of MDROs are monitored in an attempt to promote and improve infection control of MDROs, it is necessary to share monitoring data with ICU staff and provide them with continuous feedback, education on infection control of MDROs, and activities to raise awareness about the importance of infection control of MDROs. It is thought that these activities will help ICR nurses to internalize subjective norms about infection control of MDROs, influence behavioral intention, thereby leading ICR nurses to give priority to infection control of MDROs at any time in any place, and help them to practice infection control behavior for MDROs.
- In the relationship between perceived behavioral control and performance regarding infection control of MDROs, intention was found to have a partial meditating effect, and these results indicate that perceived behavioral control is a factor directly influencing performance. These findings are consistent with previous structural model studies on infection control performance of MDROs [17,23], which reported that perceived behavioral control had a direct effect on infection control performance, and it also had a partial mediating effect through intention. Perceived behavioral control refers to a high level of confidence in one’s ability to control factors as needed for performing infection control through perceiving the ease and difficulty of performing infection control against MDROs [20]. In other words, perceived behavioral control can be improved by providing support for resources needed for infection control against MDROs and removing factors hindering infection control. In a previous study, the greatest difficulty in properly performing infection control of MDROs in ICUs was found to be a lack of time [18], and these study results suggest that because ICU nurses take care of patients with high disease severity, they generally have to manage heavy workload and thus do not have a sufficient time to perform their duties while complying with MDRO infection control guidelines. The results of the 2017 (2nd) Appropriateness Evaluation of ICUs showed that the mean nurse-to-bed ratio for ICU nurses was lower in general hospitals than in tertiary general hospitals [13], and these results suggest that there is a need to consider methods for ensuring adequate nurse staffing levels in order to improve the performance of infection control against MDROs. In addition, a study on the performance of infection control against MDROs in ICU nurses of general hospitals [18] found that the level of performance was lower in isolation areas, and this lower level of performance in isolation areas was related to the fact that hospitals participating in the research failed to secure adequate space for isolation in the ICU. Actually, according to the results of the Appropriateness Evaluation of ICUs, the percentage of hospitals with the ICU equipped with isolation rooms was found to be lower in general hospitals than in tertiary general hospitals [13], and these results suggest that strict isolation of patients with MDRO infections requires appropriate administrative support. Therefore, in order to increase perceived behavioral control regarding infection control against MDROs among ICU nurses of general hospitals, it is necessary to find feasible, practical strategies to improve hindrance factors such as a lack of time, heavy workload, and a shortage of physical and human resources in relation to factors hindering infection control against MDROs that may occur in the work environment of ICUs.
- In this study, since attitude toward infection control against MDROs did not have a significant correlation with intention or performance, attitude was excluded from mediation analysis. Consistent with the results of the present study, previous studies of infection control performance among nurses [17,23] reported that attitude did not influence infection control performance. In this regard, considering that attitude refers to the level of positive or negative evaluation on MDRO infection control behavior but the performance of infection control is a moral behavior that may influence the health status of others, subjective norms are more important than a positive or negative attitude with respect to the performance of infection control [28]. According to Ajzen, behaviors with stronger social aspects are more influenced by perceived behavioral control representing the individual’s confidence about performance of behavior or by subjective norms reflecting the influence of significant people for the individual than the attitude of the individual [30].
- Infection control against MDROs is typically likely to be regarded as a low-priority task in clinical practice if there are problems such as heavy workload, a lack of time or poor accessibility to available facilities. Therefore, there is a need to develop strategies to strengthen subjective norms by presenting positive results obtainable through proper infection control against MDROs, such as a decrease in the incidence rate of MDRO infections, rather than pressuring or requiring individuals to have a positive attitude toward infection control against MDROs. It is also necessary to develop interventional programs including strategies for the enhancement of perceived behavioral control in order to improve ICU nurses’ capacity to deal with difficult situations by utilizing various resources. The development and application of such interventional programs are expected to help to enhance behavioral intention and performance regarding infection control against MDROs in ICU nurses.
Discussion
- This study attempted to investigate factors influencing the performance of infection control in ICU nurses of general hospitals based on the theory of planned behavior, and verify the mediating effect of intention, which acts as a motivation factor for performing a behavior, in order to provide basic data for the development of interventional strategies for the enhancement of infection control against MDROs.
- With respect to relationships between general characteristics of participants and infection control against MDROs, differences between attitude, subjective norm, perceived behavioral control, intention, and performance regarding infection control against MDROs according to general characteristics of participants were examined. As a result, general characteristics of participants were found to have no significant effect on variables related to infection control. In terms of relationships between major variables from the TPB, although subjective norm, perceived behavioral control, and intention regarding infection control of MDROs were significantly positively correlated with the performance of MDRO infection control. However, attitude toward infection control of MDROs did not have a significant correlation with the performance of MDRO infection control, so attitude was excluded from the analysis to verify the mediating effect of intention. The mediation analysis for the mediation effect of intention revealed that intention had a full mediating effect in the relationship between subjective norm and MDRO infection control performance, and it had a partial mediating effect in the relationship between perceived behavioral control and performance. As a result, subjective norm, perceived behavioral control, and intention were identified as factors affecting MDRO infection control performance among ICU nurses of general hospitals. These study findings suggest that in order to elicit changes in individuals’ behavior, it is necessary to enhance perceived behavioral control and subjective norms and thereby increase behavioral intention through measures such as removing factors hindering behavior, utilizing the observer effect, providing continuous feedback, and creating an organizational culture for strengthening infection control against MDROs. However, this study has limitations in generalizing research findings because participants were selected by convenience sampling among ICU nurses of six general hospitals located in a single region, and MDRO infection control behavior was studied by using data was collected not by direct observation but through a self-reported questionnaire survey. Therefore, based on the findings of the present study, this study presents the followings suggestions. First, since this study collected data from ICU nurses in general hospitals located in a single region, there is a need to conduct replication research by expanding the target region and sampling a larger population. Second, it is also necessary to develop intervention programs to enhance infection control performance of MDROs among ICU nurses in general hospitals, based on the findings of this study.
Conclusions
-
Conflict of interest
The authors declared no conflict of interest.
-
Funding
None.
-
Authors’ contributions
Kim, Nam-Sook contributed to conceptualization, methodology, project administration, visualization, writing-original draft, and investigation. Choi, So-Eun contributed to conceptualization, data curation, formal analysis, methodology, writing-review-editing, and supervision.
-
Data availability
Please contact the corresponding author for data availability.
NOTES
Acknowledgments
MDROs=Multidrug-resistant organisms; VRSA=Vancomycin–resistant Staphylococcus aureus; MRSA=Methicillin–resistant Staphylococcus aureus; VRE=Vancomycin–resistant Enterococci; CRE=Carbapenem–resistant Enterobacteriaceae; MRPA=Multidrug- resistant Pseudomonas aeruginosa; MRAB=Multidrug- resistant Acinetobacter baumannii
- 1. Lee YS, Kim HS, Yoo JS, Yoo Jl, Jung YH. Sentinel surveillance and molecular epidemiology of multidrug resistance bacteria. Korean Journal Clinical Microbiology. 2012;15(2):43–48. https://doi.org/10.5145/KJCM.2012.15.2.43Article
- 2. Siegel JD, Rhinehar E, Jackson M, Chiarello L. Management of multidrug-resistant organisms in health care settings, 2006. American Journal of Infection Control. 2007;35(10):165–193. https://doi.org/10.1016/j.ajic.2007.10.006ArticlePubMed
- 3. Maragakis LL, Perencevich EN, Cosgrove SE. Clinical and economic burden of antimicrobial resistance. Expert Review Anti-Infective Therapy. 2008;6(5):751–763. https://doi.org/10.1586/14787210.6.5.751ArticlePubMed
- 4. Barrasa-Villar JI, Aibar-Remón C, Prieto-Andrés P, Mareca-Doñate R, Moliner-Lahoz J. Impact on morbidity, mortality, and length of stay of hospital-acquired infections by resistant microorganisms. Clinical Infectious Diseases. 2017;65(4):644–52. https://doi.org/10.1093/cid/cix411ArticlePubMed
- 5. Korea Centers for Disease Control and Prevention. 2020 Case definitions national notifiable infectious diseases[Internet] Cheongju: Korea Centers for Disease Control and Prevention. 2019 [cited 2020 Jul 02]. Available from: https://www.kdca.go.kr/board/board.es?mid=a20507020000&bid=0019
- 6. Korea Centers for Disease Control and Prevention. 2020 Healthcare-associated infection control guideline[Internet] Cheongju: Korea Centers for Disease Control and Prevention. 2019 [cited 2020 Feb 26]. Available from: https://www.kdca.go.kr/board/board.es?mid=a20507020000&bid=0019
- 7. Korean Society for Healthcare-associated infection Control and Prevention. Infection control and prevention in healthcare facilities. 5th ed. Seoul: Hanmibook; 2017. p. 985.
- 8. Barsanti MC, Woeltje KF. Infection prevention in the intensive care unit. Infectious Disease Clinics of North America. 2009;23(3):703–25. ArticlePubMed
- 9. Lee YS, Kim YA, Song WK, Lee HM, Lee HS, Jang SJ, et al. Recent trends in antimicrobial resistance in intensive care units in Korea. Korean Journal of Nosocomial Infection Control. 2014;19(1):29–36. https://doi.org/10.14192/kjnic.2014.19.1.29Article
- 10. Oh HS. National survey on nurses’ knowledge of infection control in general hospitals and analysis of variables to impact on their knowledge. Journal of Nosocomial Infection control. 2005;10(2):78–86.
- 11. Oh HS. Current status of infection control of multidrug resistant organisms in hospitals with more than 200 beds in the Republic of Korea. The Korean Journal of Health Service Management. 2014;8(4):163–173. https://doi.org/10.12811/kshsm.2014.8.4.163Article
- 12. Jeong SY, Kim OS, Lee JY. The status of healthcare-associated infection control among healthcare facilities in Korea. Journal of Digital Convergence. 2014;12(5):353–366. Article
- 13. Health Insurance Review & Assessment Service. Results of adequacy test for intensive care unit in 2017.2nd[Internet] Wonju: Health Insurance Review & Assessment Service. 2018[cited 2018 Aug 23]. Available from: https://www.hira.or.kr/ra/eval/getDiagEvlView.do?pgmid=HIRAA030004000100&WT.ac=%EB%B3%91%EC%9B%90%ED%8F%89%EA%B0%80%EB%B0%94%EB%A1%9C%EA%B0%80%EA%B8%B0
- 14. Song JO. Perception of multidrug-resistant organisms control in ICU nurses [master’s thesis]. [Seoul]: Yonsei University. 2013 58p
- 15. Shon JA, Park JH. Knowledge and compliance level of the multi-drug resistant organisms of ICU nurses. Journal of the Korea Academia-Industrial Cooperation Society. 2016;17(7):280–292. http://doi.org/10.5762/KAIS.2016.17.7.280Article
- 16. Kim SY, Cha CY. Factors related to the management of multi-drug resistant organisms among intensive care unit nurses: an application of the health belief model. Journal of Korean Academy Fundamentals of Nursing. 2015;22(3):268–276. https://doi.org/10.7739/jkafn.2015.22.3.268Article
- 17. Gu JE, Ha YK, Hwang SH, Gong KH. Path analysis of performance of multi-drug resistant organisms management guidelines among intensive care unit nurses: with focus on the theory of planned behavior and patient safety culture. Journal of Korean Critical Care Nursing. 2018;11(1):89–100.
- 18. Kim JH, Lim KH. The factors influencing compliance of multidrug-resistant organism infection control in intensive care unit nurses. Korean Journal of Adult Nursing. 2015;27(3):325–336. http://doi.org/10.7475/kjan.2015.27.3.325Article
- 19. Park YM, Park HS, Park KY. Factors influencing level of awareness and compliance with vancomycin-resistant enterococcus infection control among nurses in intensive care units. Journal of Korean Academy of Fundamentals of Nursing. 2008;15(4):531–538.
- 20. Ajzen I. The theory of planned behavior. Organizational Behavior and Human Decision Processes. 1991;50(2):179–211. https://doi.org/10.1016/0749-5978(91)90020-TArticle
- 21. Jeong SY, Kim OS. The structural model of hand hygiene behavior for the prevention of healthcare-associated infection in hospital nurses. Korean Journal Adult Nursing. 2012;24(2):119–129. http://doi.org/10.7475/kjan.2012.24.2.119Article
- 22. Kim SM. An analysis about the performance of the clinical nurses in nosocomial infection management by applying the theory of planned behavior [master’s thesis]. [Daejeon]: Chung Nam National University. 2004 79p
- 23. Moon JE, Song MO. A convergence study about the performance of healthcare-associated infection control guidelines of hospital nurses-based on the theory of planned behavior. Journal of the Korea Convergence Society. 2017;8(5):117–125. https://doi.org/10.15207/JKCS.2017.8.5.117Article
- 24. Baron RM, Kenny DA. The moderator-mediator variable distinction in social psychological research: conceptual, strategic, and statistical considerations. Journal of Personality and Social Psychology. 1986;51(6):1173–1182. https://doi.org/10.1037//0022-3514.51.6.1173ArticlePubMed
- 25. Sobel ME. Asymptotic confidence intervals for indirect effects in structural equation models. Sociological Methodology. 1982;13:290–312. https://doi.org/10.2307/270723Article
- 26. Cha KS, Shin MJ, Lee JY, Chun HK. The Role of infection control nurse during emerging infectious disease epidemic: focusing on the middle east respiratory syndrome. Korean Journal of Healthcare-Associated Infection Control and Prevention. 2017;22(1):31–41. https://doi.org/10.14192/kjhaicp.2017.22.1.31Article
- 27. Ministry of Legislation. Enforcement rules of the medical law. Enforcement rules of the medical law article 43(1), article 43(2), article 43(3) [Internet]. Korea: Ministry of Legislation. 2016 [cited 2023 Feb 18]. Available from: https://www.law.go.kr/LSW//lsInfoP.do?lsiSeq=188968&ancYd=20161229&ancNo=00458&efYd=20161230&nwJoYnInfo=N&efGubun=Y&chrClsCd=010202&ancYnChk=0#0000
- 28. Lee MR, So HY, Cho MK. Determinants of nurses handwashing practice. The Journal of Korean Academic Society of Adult Nursing. 2005;17(2):268–275.
- 29. Kweon OM, Park ES, Lee DS, Lee JH, Ha EJ, Yong DE, et al. A three-year study of the effectiveness of hand-hygiene protocol implementation at a university hospital. Korean Journal Nosocomial Infection Control. 2012;17(2):53–60.
- 30. Ajzen I. Attitudes, personality, and behavior. 2nd ed. NY: Open University Press. 2005 p. 191
 PubReader
PubReader ePub Link
ePub Link Cite
Cite