Articles
- Page Path
- HOME > Res Community Public Health Nurs > Volume 34(4); 2023 > Article
-
Original Article
- Good subjective health status and health-related quality of life in people with chronic kidney disease: A secondary analysis using the Korea National Health and Nutritional Examination Survey in 2019 and 2020
-
Jena Lee1
 , Yujin Suh2
, Yujin Suh2 -
Research in Community and Public Health Nursing 2023;34(4):255-266.
DOI: https://doi.org/10.12799/rcphn.2023.00262
Published online: December 29, 2023
1Lecturer, College of Nursing, JEI University, Incheon, Korea
2Assistant Professor, College of Nursing, Healthcare sciences and the Human Ecology, Dong-eui University, Busan, Korea
- Corresponding author: Suh, Yujin College of Nursing, Healthcare sciences and the Human Ecology, Dong-eui University, 176 Eomgwangro, Busanjin-gu, Busan, South Korea, 47340 Tel: +82-51-890-4219, Fax: 0504-240-1163, E-mail: yugibabe@deu.ac.kr
Copyright © 2023 Korean Academy of Community Health Nursing
This is an Open Access article distributed under the terms of the Creative Commons Attribution NoDerivs License. (http://creativecommons.org/licenses/by-nd/4.0) which allows readers to disseminate and reuse the article, as well as share and reuse the scientific material. It does not permit the creation of derivative works without specific permission.
- 1,089 Views
- 36 Download
Abstract
-
Purpose
- This cross-sectional study aimed to describe subjective health status of people with chronic kidney disease (CKD), identify factors that affect good subjective health status and investigate the relationship between good subjective health status and health-related quality of life (HRQOL) in people with CKD.
-
Methods
- This secondary analysis utilized data from the Korean National Health and Nutrition Examination Survey in 2019-2020. Participants (N=295) had an eGFR of ≤59 mL/min/1.73 m2. Descriptive and inferential statistics were used to analyze the data. Univariate and multivariate logistic regression analyses were performed to identify factors affecting good subjective health status and examine the association between good subjective health status and HRQOL.
-
Results
- Among all participants, 61.4% had good subjective health status, and the HRQOL index was 0.88 in people with CKD. Household income, activity limitation, stress, and the number of comorbidities in people with CKD were associated with good subjective health status. People with better subjective health status were more likely to be satisfied with self-care, usual activities, and pain/discomfort in HRQOL.
-
Conclusion
- Good subjective health status is associated with better HRQOL. Therefore, subjective health status should be assessed early, and a nursing intervention program should be developed considering factors that can improve subjective health status in people with CKD.
- 1. Background
- Chronic kidney disease (CKD) is defined as the presence of an estimated Glomerular Filtration Rate (eGFR) of 59ml/min/1.73m2 or less that persists for 3 months or more [1], and the prevalence of CKD is estimated to be around 11% of the world’s population [2]. In Korea, according to data from 2021 National Health Statistics Reports, the prevalence of CKD is 8.4% in people aged 19 and older and 38.5% in people aged 60 and older [2]. In the U.S., the prevalence of CKD is reported to be 14% in the total population and 33.7% in people aged 65 and older [3]. In Korea, with rapid population aging, the prevalence of CKD in the elderly population is relatively higher than in other countries, leading to an increase in social medical expenditure and mortality, so CKD is emerging as a national health problem [2,4,5].
- Subjective health status is an indicator of the overall assessment of physical, physiological and psychosocial health, and it reflects a complex notion of health [4-8]. It is currently being used as the most common and highly predictive indicator of health status despite the limitation that individuals may overrate or underrate their own health through subjective assessment [8-10].
- For CKD patients, to prevent uremia due to impaired kidney function, they are required to steadily perform self-care as well as health-related activities such as medication adherence, exercise therapy, and dietary regimen, based on the proper perception and evaluation of their health status [4]. However, in CKD patients, the mortality rate was reported to be 2-3 times higher in the group with poor subjective health status than in the group with good subjective health status [5]. In addition, emergency situations such as hyperphosphatemia, hyperkalemia, and metabolic acidosis occur frequently in CKD patients due to ingrained lifestyle habits and the failure of the kidneys to remove waste from the body [4-8]. On the other hand, patients with good subjective health status were found to show voluntary and cooperative behaviors suitable for given situations to maintain or promote health [9,10]. This was attributed to the fact that since subjective health status includes well-being, the group with good subjective health status showed an active attitude toward both interactions with medical staff and modifying lifestyle[5-10].
- In a study of 366 CKD patients conducted in Korea [4], 42.9% of CKD patients rated their subjective health status as poor, and this result is similar to 43.1% reported by a study of 1,268 nephrology patients in the U.S. [7]. Generally, 47-53% of CKD patients are reported to assess their subjective health status as poor, and it has been found that CKD patients are more likely to evaluate subjective health status negatively than patients with other chronic diseases [7].
- According to previous studies, factors that may affect subjective health status in CKD patients include sociodemographic indicators, such as gender [4,5], age [5,7], household income level [4], education level [4,5], the presence of household members [4], as well as health-related indicators, such as activity limitation [7,8], the frequency of alcohol consumption [4,5,11], stress [7], the number of comorbidities [5,10,11], and eGFR [5,7]
- CKD poses a threat to life regarding the symptoms of uremia, and it is accompanied by a combination of various problems, such as fear of death, loss of the function of a body part, pain, financial difficulties, and emotional problems such as stress, depression, and anxiety, so it has a negative impact on quality of life [4,5,7,8,10,11]. In overseas studies that assessed quality of life in CKD patients using EuroQol 5-Dimension (EQ-5D), the score for quality of life was reported as 0.81 points [12] and 0.75 points [13], and these results indicate that the level of quality of life in CKD patients [12,13] is relatively lower, compared to 0.82 points in a domestic study of patients with complex chronic diseases [14].
- According to previous studies, the presence of a chronic disease may reduce the level of subjective health status [6], but if individuals perceive their subjective health status positively, it can give them a strong motivation for health management, and lead individuals to have a positive self-image [15-18]. Regarding previous studies on the impact of subjective health status on health-related quality of life in CKD patients, a study of patients with stages 4-5 CKD found that patients with better subjective health status were 2.88 times more likely to show improvement in health-related quality of life (HRQOL) [6]. Similarly, Lee & Chun [15] also reported that subjective health perception had a significant direct impact on quality of life in stroke patients, and a better subjective health perception was associated with a higher level of the practice of both health-promoting activities and activities promoting changes in individual habits as well as environmental changes. Therefore, since quality of life in CKD patients is not determined only by physical aspects, it is necessary to consider the meaning and influencing factors of subjective health status. However, although foreign researchers studied the meaning of subjective health status as a health indicator in CKD patients [6,7,8,10,11], and reported that subjective health status is an important factor affecting HRQOL, and there is a need to investigate the impact of subjective health status [6,19], in Korea, despite the increased awareness of the importance of subjective health status, there have been few studies that supported the relationship between subjective health status and quality of life. Therefore, this study attempted to investigate influencing factors for good subjective health status in CKD patients by using data from the 8th (2019-2020) National Health and Nutrition Examination Survey with the aim of providing basic data for the development of nursing interventions for the promotion of HRQOL.
- 2. Objectives
- This study aimed to investigate subjective health status and health-related quality in patients with CKD, identify influencing factors for good subjective health status, and examine the effects of good subjective health status on HRQOL.
Introduction
- 1. Study design
- The present study is a secondary data analysis study conducted using raw data collected in the first and second years (2019-2020) of the 8th (2019-2020) National Health and Nutrition Examination Survey (NHANES) [20] in order to identify influencing factors for good subjective health status, and examine the effects of good subjective health status on HRQOL among patients with CKD.
- 2. Participants
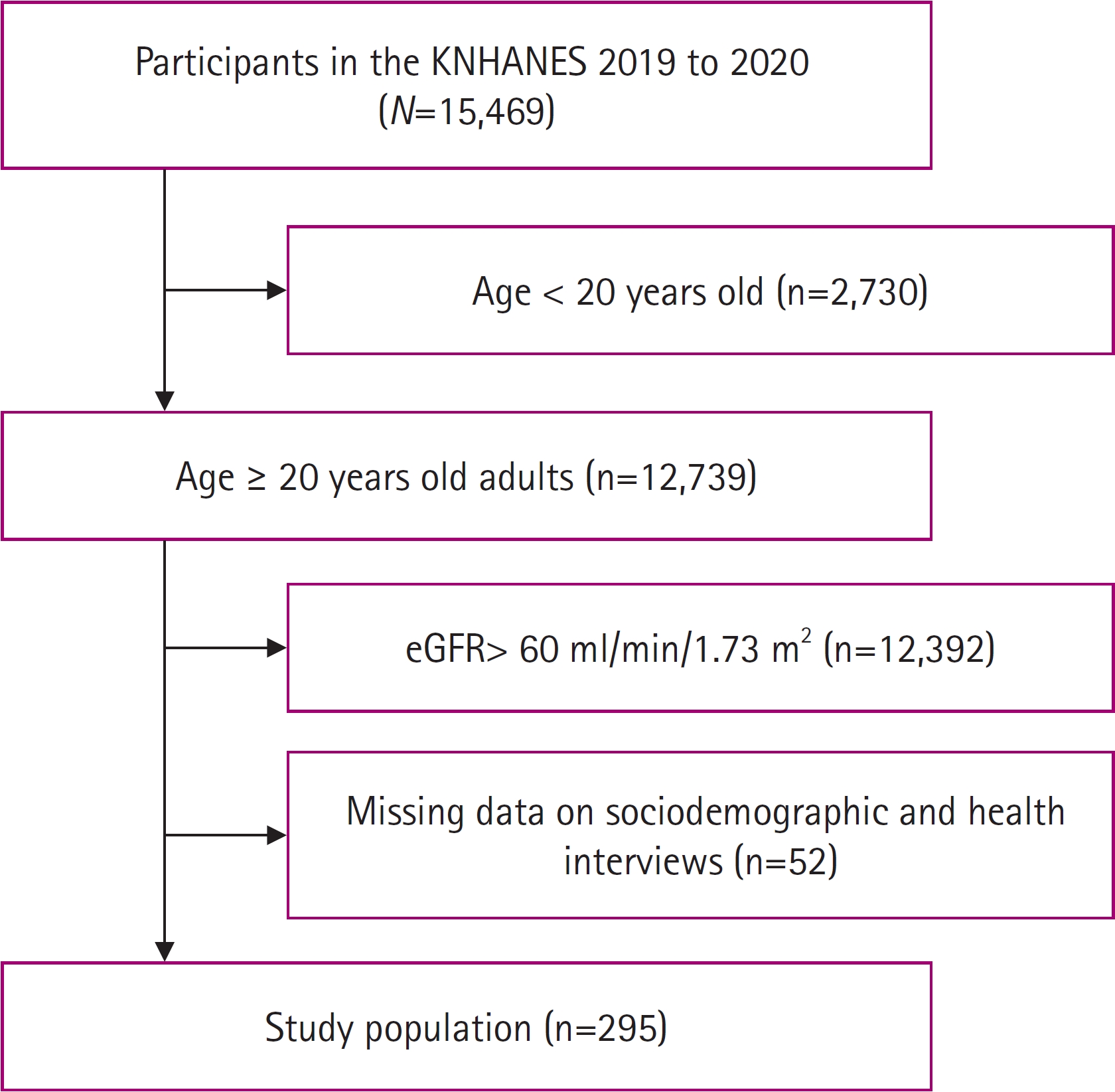
- The participants of this study were selected from the participants of the 8th (2019-2020) National Health and Nutrition Examination Survey (NHANES), which was a general population survey conducted by a stratified sampling method. Among 15,469 participants of the 8th (2019-2020) NHANES, 12,739 adults aged 19 or older were first extracted. Then, out of the 12,739 people, 347 patients with stages 3-5 CKD (≤eGFR 59ml/min/1.73m2) who needed tests and treatment for complications [1] were extracted. Then, 259 patients were finally selected as participants by excluding people with missing data in sociodemographic data and responses to health questionnaire items (Figure 1).
- 3. Measures
- The general characteristics of participants examined in this study are as follows: gender, age, household income level, education level, and the presence of household members.
- The health-related characteristics of participants examined in this study were activity limitation, alcohol drinking frequency, stress, the number of comorbidities, and eGFR. eGFR was calculated by the CKD Epidemiology Collaboration (CKD-EPI) equation using serum creatinine values. For females, if the serum creatinine level is ≤0.7 mg/dL, GFR is calculated as follows: GFR=142×(sCr/0.7)-0.241×(0.9938)age×1.012; if the serum creatinine level is >0.7 mg/dL, GFR is calculated as follows: GFR=142×(sCr/0.7)-1.200× (0.9938)age× 1.012. For males, if the serum creatinine level is ≤0.9 mg/dL, GFR is calculated as follows: GFR= 142×(sCr/0.9)-0.302×(0.9938)age; and if the serum creatinine level >0.9mg/dL, GFR is obtained as follows: GFR= 142×(sCr/0.9)-0.302×(0.9938)age [1]. In this study, according to the definition presented by the National Kidney Foundation of the U.S., the Stages 3-5 of CKD were defined as follows: Stage 3: eGFR of 30-59 ml/min/1.73m2; Stage 4: eGFR of 15-29 ml/min/1.73m2; Stage 5: eGFR <15 ml/min/1.73m2 [1].
- Subjective health status was measured on a 5-point scale (‘very good, good, moderate, poor, and very poor’) by using the question “What do you think of your usual health?” In this study, based on a previous study [22], to increase statistical power and the accuracy of interpretations, the level of subjective health status was dichotomously divided. In other words, the responses of ‘very good, good, and moderate’ were categorized as ‘good’, and the responses of ‘poor and very poor’ were categorized as ‘poor.’ In addition, Ambagtsheer et al. [23] reported that questionnaire items on subjective health status were found to have a sensitivity value of 62.5%, a specificity value of 93.6%, positive predictive value of 67.5%, and a negative predictive value of 92.2%.
- HRQOL was measured using a Korean version of the EuroQol-5 Dimension (EQ-5D). This scale is composed of 5 subdomains: mobility, self-care, usual activities, pain/discomfort, and anxiety/depression. Each subdomain was measured on a 3-point scale (‘no problems’, ‘some problems’, and ‘severe problems’). In this study, the level of quality of life was dichotomously divided into ‘no problems’ and ‘some problems’ by categorizing ‘some problems’ and ‘severe problems’ into ‘some problems.’ The Korean Disease Control and Prevention Center applies a weighting formula to calculate the EQ-5D index values for Koreans. If the scores of all the five items is 1, the EQ-5D index value becomes 1, and if the scores of all the five items are 3, which indicates the poorest health status, the EQ-5D index value is adjusted to -0.17 [23]. Regarding the reliability of the tool, Limin et al. [24] reported that the value of overall percent agreement was calculated as 86-94%, the value of kappa as 0.79-0.85, and the intraclass correlation coefficient as 0.98
- 4. Data collection and analysis
- The data collection of the first and second years (2019~2020) of the 8th National Health and Nutrition Examination Survey was carried out from January 1, 2019 to December 31, 2020. The raw data was collected by a health questionnaire survey, health examination survey, and a nutrition survey. The health questionnaire survey was conducted in the form of a self-report survey on the domains of health behaviors such as smoking and drinking, and health check-ups were performed by methods such as physical measurement and blood tests. The NHANES data were collected by selecting the samples that are representative of the entire population of Korea by a probability sampling method, and statistical analysis for complex sampling data was performed. This study analyzed the data collected in 2019 and 2020, and used the integrated weight of the data collected for two years. Also, data analysis was performed by specifying the stratification variables and cluster variables presented by the Korea Disease Control and Prevention Agency. Data analysis was conducted using SPSS/Win 27.0 (IBM Corp., Armonk, NY, USA), and the sociodemographic characteristics, subjective health status, and HRQOL of the participants were analyzed using descriptive statistics. Based on a previous study [25], to increase statistical predictive power, a univariate logistic regression analysis was first performed to identify factors affecting good subjective health status in the participants. Then, a multivariate logistic regression analysis was conducted using statistically significant variables identified through the univariate logistic regression analysis. In addition, to examine the impact of good subjective status on HRQOL, a univariate logistic regression analysis was performed, and only statistically significant variables among the subdomains of HRQOL were entered into a multivariate logistic regression analysis. This regression analysis was conducted after controlling for variables affecting HRQOL, such as gender, age, household income level, educational level, the presence of household members, activity limitation, the frequency of alcohol consumption, stress, the number of comorbidities, and eGFR. Regarding subjective health status, the odds ratio for good subjective health status was estimated by using poor subjective health status as the reference category. As for quality of life, the odds ratio for ‘no problems’ was estimated by using ‘some problems’ as the reference category. The odds ratio (OR) and 95% confidence interval (CI) were calculated using the multivariate logistic regression analysis, and the significance level for statistical tests was set at < .05.
- 5. Ethical considerations
- This study received a review exemption determination from the Public Institutional Review Board designated by the Ministry of Health and Welfare (IRB No.: P01-202306-01-008), and this research was conducted after obtaining approval regarding the use of data from the National Health and Nutrition Examination Survey (NHANES) after submitting the non-disclosure (confidentiality) agreement and the data use agreement in accordance with the raw data use procedures of the NHANES of the Korea Disease Prevention and Control Agency.
Methods
1) Sociodemographic characteristics
2) Heath-related characteristics
3) Subjective health status
4) Health-related quality of life (HRQOL)
- 1. Sociodemographic and health-related characteristics of CKD patients
- With respect to the sociodemographic characteristics of the participants, the participants of this study consisted of 162 males (54.9%), and 133 females (45.1%), so the proportion of males was greater. The mean age of the participants was 70.74 years, and the 70-79 age group made up the largest proportion (41.4%). As for household income level, people in the low household income group made up 49.8% of the participants. Regarding education level, people with the education level of middle-school graduation or lower accounted for 69.1%. For the number of household members, people with one or more household members constituted 74.9% of the participants. With respect to health-related characteristics, 243 persons (82.3%) had no activity limitations, and 153 persons (51.9%) were nondrinkers. Regarding the stress level, people with a low level of stress accounted for the largest proportion (85.1%). In terms of the number of comorbidities, patients with three comorbidities were 145 persons (49.2%), accounting for the largest proportion. The mean value of eGFR was 47.70 ml/min/1.73m2, and the patients with an eGFR of 30-59 ml/min/1.73m2 (stage 3 CKD) were 269 persons (91.2%), taking up the vast majority of the participants. As for subjective health status, patients with good subjective health status were 181 persons (61.4%). The mean score for HRQOL was 0.88 points, and the patients who perceived that they had ‘some problems with HRQOL’ were 167 persons (56.6%), accounting for a relatively high proportion (Table 1).
- 2. Factors affecting good subjective health status in CKD patients
- To identify factors affecting good subjective health status in CKD patients, univariate and multivariate logistic regression analyses were conducted. First, as a result of a univariate logistic regression analysis, the high household income group was found to better subjective health status than the low household income group (95% CI=1.17~8.40, p=.023). Also, the group with no activity limitation was shown to have better subjective health status than the group with activity limitation (95% CI=3.53~18.75, p<.001). The group of people drinking alcohol less than 2 times per week was found to have better subjective health status than the group of nondrinkers (95% CI=0.92~4.45, p=.011). Also, the group with a low level of stress was shown to have better subjective health status than the group with a high level of stress (95% CI=1.28~5.46, p=.009). Additionally, the group with one comorbidity (95% CI=1.71~19.63, p=.005) and the group with no comorbidities (95% CI=1.71~19.63, p=.005) were found to have better subjective health status than the group with three comorbidities.
- A multivariate logistic regression analysis was performed by entering variables identified as significant variables in the univariate logistic regression analysis, such as household income level, activity limitation, the frequently of drinking alcohol, stress, and the number of comorbidities. As a result, the high household income group was 2.55 times more likely to have good subjective health status than the low household income group (95% CI=1.05~6.21, p=.040). The group with no activity limitation was 6.20 times more likely to have good subjective health status than the group with activity limitation (95% CI=2.43~15.85, p<.001). Also, the group with a low level of stress was 2.46 times more likely to have good subjective health status than the group with a high level of stress (95% CI=1.08~5.61, p=.032), and the group with no comorbidities was 5.11 times more likely to have good subjective health status than the group with 3 comorbidities (95% CI=1.60~16.32, p=.006). However, in the case of the frequency of drinking alcohol, there were no significant differences in subjective health status between the nondrinker group and the group of people drinking two or more times per week (95% CI=0.65~3.23, p=.367) and between the nondrinker group and the group of people drinking less than two times per week (95% CI=0.87~2.86, p=.132) (Table 2)
- 3. The impact of good subjective health status on HRQOL in CKD patients
- To examine the impact of good subjective health status on HRQOL, univariate and multivariate logistic regression analyses were conducted, and the results showed that subjective health status had a significant effect on self-care, usual activities, and pain/discomfort among the subdomains of HRQOL.
- First, a univariate logistic regression analysis for the effects of subjective health status on the subdomains of HRQOL was performed. As a result, compared to the poor subjective health status group, the good subjective health status group was found to be more likely to have no problems in self-care(95% CI=1.77~9.87, p=.001), usual activities(95% CI=1.64~6.40, p=.001), pain/ discomfort (95% CI=1.56~4.83, p<.001), and anxiety/depression (95% CI=1.42~5.81, p=.003), which are the subdomains of HRQOL
- Next, a multivariate logistic regression analysis was conducted after controlling for variables influencing HRQOL, such as age, gender, household income level, education level, the presence of household members, activity limitation, stress, the number of comorbidities, and eGFR. As a result, the good subjective health status group was found to be more likely to have no health problems in the subdomains of HRQOL than the poor subjective health status group. More specifically, compared to the poor subjective health status group, the good subjective health status group was 3.03 times more likely to have no problems in self-care (95% CI=1.12~8.19, p=.029), and was 2.52 times more likely to have no problems in usual activities (95% CI=1.11~5.71, p=.027). Also, the good subjective health status group was 1.99 times more likely to have no problems in pain/discomfort (95% CI=1.04~3.83, p=.039). However, subjective health status was found to have no significant effect on anxiety/depression (95% CI=0.72~3.36, p=.264) (Table 3).
Results
- In this study, 61.4% of participants rated their subjective health status as good. This percentage is higher than the results of some prior studies. Specifically, studies by Yoo, Kim & Kim [4] and Lee et al. [7] on CKD patients reported the proportion of patients with good subjective health status as 57.1% and 56.9%, respectively. These differences in research results may be attributed to the findings of previous studies [4,5] that there were significant gender differences in subjective health status, and males evaluated subjective health status more positively. Actually, in this connection, it has been reported that women tend to show higher prevalence rates of chronic diseases and higher healthcare utilization, indicating that women actually have more vulnerable physical health than men, and women also tend to be more sensitive to the same health problems and evaluate their health negatively [26]. In this study, the proportion of male participants (54.8%) was higher than that of females, and it is considered necessary to conduct further research on the impact of gender differences in biological and sociocultural health attitudes on subjective health status.
- In this study, the score for quality of life in CKD patients was 0.88 points, and this is slightly higher than the results of some previous studies [12,13]. In the prior studies of CKD patients, Jafari et al. [12] and Wen et al. [13] measured quality of life in patients receiving hemodialysis among CKD patients, and they reported the score for quality of life as 0.82 points and 0.75 points, respectively. These differences in research results may be attributed to the fact that the previous studies [12,13] enrolled CKD patients receiving hemodialysis as the participants, and did not precisely present the stages of CKD of patients, and information on whether each individual is receiving dialysis or not is not available in the NHANES data. However, a study of 3216 patients with chronic diseases in Korea [14] reported the score for quality of life as 0.82 points, and a study of 1932 patients with chronic diseases conducted in Singapore [27] reported the score for quality of life as 0.94 points. In terms of quality of life in patients with chronic diseases, the results of this study are considered similar to these two previous studies.
- In this study, factors affecting good subjective health status in CKD patients were identified as household income level, activity limitation, stress, and the number of comorbidities. In addition, a high household income level, the absence of activity limitation, less stress, and a fewer number of comorbidities were associated with better subjective health status. More specifically, in this study, the high household income group was 2.55 times more likely to have good subjective health status than the low household income group. Similarly, Yoo, Kim & Kim [4] reported that the group with a household income less than the mean value is 1.19 times more likely to have poor subjective health status than the group with a household income level equal to or higher than the mean value. Thus, regarding the results about the household income level, the results of this study support the findings of previous studies. The above-mentioned findings about the household income level can be attributed to the fact that higher household income levels are associated with higher accessibility to appropriate healthcare and prevention services, and lower household income levels are linked to indifference to health checkups and the maintenance of unhealthful health behaviors [5,10]. With respect to activity limitation, in this study, the group with less activity limitation was 6.20 times more likely to have good subjective health status, and this result was similar to the findings of previous studies. For example, Lee et al. [7] reported that people with less limitation on activities of daily living (ADL) are 8.29 times more likely to have good subjective health status. In relation to activity limitation, decreased physical function and reduced independence in daily life were reported to be associated with poor subjective health status as well as related physical symptoms in CKD patients, so they were found to be major variables related to subjective health status [7,8]. As for the frequency of drinking, in this study, the results of multivariate logistic regression analysis showed that it did not have a significant effect. On the other hand, Kim & Kim [4] reported that people drinking 2 or more times per week are 0.87 times likely to have poor subjective health status. Similarly, Ko et al. [5] reported the likelihood as 0.71 times, and Robinson-Cohen et al. [11] reported it as 0.7 times. Regarding these results, it has been suggested that the moderate drinking group is more likely to rate their subjective health status as good due to the finding that since moderate drinking (consumption of about 30g of alcohol) increases high density lipoprotein cholesterol(HDL) levels and reduces platelet aggregation, it helps to prevent cardiovascular diseases [21]. However, according to in a recent study [28], there is insufficient evidence to medically support the health benefits of drinking, and drinking may rather increase risks for binge drinking, depression, and complications of diseases. Therefore, further research is required to analyze the effects of the frequency of alcohol consumption. Regarding stress, in this study, patients with lower stress levels were 2.46 times more likely to assess their subjective health status as good. In agreement with this study, Lee et al. [7] reported that individuals with lower stress are 1.67 times more likely to perceive subjective health status as good. In particular, according to previous studies, stress caused by illness negatively affects physical and mental health, and if the patient perceives stress, the endocrine system may be disturbed for physical adaptation to stress, which may result in decreased immune responses [7,8]. In addition, it has been reported that changes in daily life due to CKD may be associated with the changes of body image and self-concept and even treatment non-adherence as well as the burden of disease, and these findings indicate the importance of stress management [7,8]. With respect to the number of comorbidities, in this study, the absence of comorbidities was associated with a 5.1 times greater likelihood of good subjective health status. This finding is consistent with a study by Swetalina et al. [10], which reported that the absence of comorbidities was associated with a 5.1 times greater likelihood of good subjective health status. Ko et al. [5] reported that the presence of diabetes in CKD patients was associated with a 1.65 times greater likelihood of poor subjective health status, and the presence of hypertension was linked to a 1.29 times greater likelihood of poor subjective health status. Likewise, in a previous study of CKD patients, Robinson-Cohen et al. [11] also found that the group with hypertension and the group with diabetes are 2.23 times and 2.79 times more likely to have poor subjective health status, respectively, compared to the group without hypertension or diabetes. Therefore these findings indicate that hypertension and diabetes, which are reported to be the most common comorbidities of CKD patients [2], are significant influencing factors for the subjective health status of CKD patients [5,11]. As the number of comorbidities increases, healthcare utilization and medical cost increase which leads to an financial burden of patients [5]. In particular, as the increase of comorbidities entails the increase of dietary regimen, exercise therapy, and drug regimen that patients need to manage for themselves, and if patients neglect disease management, it may result in the occurrence of complications or the aggravation of disease. For these reasons, the number of comorbidities has been reported as a major influencing factor of subjective health status [10,11].
- In this study, In CKD patients, the good subjective health status group was associated with a greater likelihood of having no health problems in the subdomains of HRQOL. Specifically, the likelihood of having no health problems was 3.03 times, 2.52 times, and 1.99 times greater, respectively, for self-care, usual activities, and pain/discomfort among the subdomains of HRQOL. Similarly, Grove et al. [6] measured quality of life in CKD patients by using the 36-item Short Form Health Survey (SF-36), and found that quality of life is 2.88 times more likely to be promoted in better subjective health status. Self-care is to actively participate in disease treatment, spontaneously identify one’s own health problems, and practice the knowledge, education, and skills necessary for health management, and it has been reported that the comprehensive examination and evaluation of one’s health status are prerequisites for self-care [24,27,29]. In this regard, it has been reported that a more positive perception of one’s health status is more likely to motivate people to change ingrained lifestyle habits in a desirable direction [27,29]. These research results about self-care suggest that good subjective health status is also an important factor for the practice of self-care. In addition, regarding usual activities, CKD patients reported that decreased renal function may lead to decreased in muscular and skeletal function [7], but a previous study reported that if individuals’ health evaluation is positive, CKD patients are likely to have a higher level of satisfaction with maintaining and performing independent daily activities, including activities related to diet, clothing, and residence [13]. These findings are thought to suggest that although the ability to perform ADL has been decreased, good subjective health status may promote social relationships such as leisure activities and social gatherings, and thus, it leads patients to experience more psychological stability [14]. Therefore, even among patients with the same disease and the same symptoms, the level of satisfaction with daily life may be different among individuals, so there is a need to consider personalized intervention preventions. With respect to pain/discomfort, it was difficult to find previous studies on the relationship between subjective health status and pain as a subdomain of quality of life. However, the results of this study suggest that since the perception of pain is based on individuals’ subjective emotional experiences, it is closely related to psychological and emotional environments, and positive health perceptions and attitudes are important for quality of life, including pain. In particular, the decrease in kidney function causes muscle and nerve damage, which are accompanied by discomfort such as muscle atrophy, muscle cramps, and pain [8,10,28]. Considering this fact, there is a need to analyze the relationship of health assessment including these physical symptoms with pain/discomfort experienced in daily life in future studies. The results of this study suggest that subjective health status has a significant impact on quality of life, and it may have a greater effect on quality of life than the presence of illness among CKD patients. Although it is not easy for CKD patients to change their ingrained lifestyle habits, it is noteworthy that the positive evaluation of health status is likely to lead them to recognize the importance of health as the subjects of life, and motivate them to practice more health-promoting behaviors. Therefore, it is necessary to actively utilize the findings about the impact of the positive evaluation of health status in the interventions for CKD patients. More specifically, the local community should help CKD patients practice health-related behaviors to maintain their health on their own by implementing an early assessment of subjective health status, and promoting positive subjective health status, and these efforts are expected to contribute to the improvement of CKD patients’ self-care ability and well-being.
Discussion
- This study attempted to investigate factors affecting good subjective health status and the effects of good subjective health status on health-related quality of life (HRQOL) in CKD patients. As a result, factors affecting good subjective health status were identified as a high household income level, the absence of activity limitation, a low level of stress, and a small number of comorbidities. In addition, the results of this study showed that CKD patients with better subjective health status are more likely to have higher satisfaction in self-care, usual activities, and pain/discomfort among the subdomains of HRQOL. Based on the results of this study, the following suggestions are presented. First, it is necessary to verify the predictability of subjective health status in CKD patients by including objective health measurement variables such as the presence of dialysis, the treatment history of comorbidities, and the presence of the experience of hospital admission. Second, although this study elucidated the relationship between subjective health status and HRQOL in CKD patients, this study is a secondary data analysis and thus had limitations in investigating causal relationships. For this reason, further research is required to clarify the causal relationships between subjective health status and HRQOL. Third, considering that the improvement of quality of life is the ultimate goal of CKD patients, to achieve the improvement of quality of life in CKD patients, a follow-up study is required to develop nursing intervention programs that can implement the early assessment of subjective health status and consider and reflect the factors for promoting subjective health status based on the assessment results.
Conclusions
-
Conflict of interest
The authors declared no conflict of interest.
-
Funding
None.
-
Authors’ contributions
Lee, Jena contributed to conceptualization, data curation, formal analysis, funding acquisition, methodology, project administration, visualization, writing - original draft, review & editing, investigation, resources, software, supervision, and validation. Suh, Yujin contributed to conceptualization, data curation, formal analysis, funding acquisition, methodology, project management, visualization, writing-original draft, review & editing, investigation, resources, software, supervision, and validation.
-
Data availability
Please contact the corresponding author for data availability.
NOTES
Acknowledgments

CI=confidence interval; OR=odds ratio; ref=reference; SHS=subjective health status; HRQOL=health-related quality of life.
Note. Adjusted variable: gender, age, household income, education, household members, activity limitation, alcohol drinking, stress, number of comorbidities, and estimated Glomerular Filtration Rate(eGFR).
Reference group of SHS: poor, Comparison group of SHS: good. Reference group of HRQOL: having problem, Comparison group of HRQOL: no problem.
- 1. National Kidney Foundation. Kidney Failure Risk Factor: Estimated Glomerular Filtration Rate (eGFR)(2021) [Internet]. New York: National Kidney Foundation. 2023 [cited 2023 Apr 26]. Available from: https://www.kidney.org/content/kidney-failure-risk-factor-estimated-glomerular- filtration-rate-egfr
- 2. The Korea Disease Control and Prevention Agency. Trends in the prevalence of chronic kidney disease. Public Health Weekly Report. 2023;16(8):238–239. https://doi.org/10.56786/PHWR.2023.16.8.3Article
- 3. Centers for Disease Control and Prevention. Chronic Kidney Disease in the United States, 2023 (2023) [Internet]. Atlanta: Centers for Disease Control and Prevention. 2023 [cited 2023 Apr 26]. Available from: https://www.cdc.gov/kidneydisease/publications-resources/ckd-national-facts.html
- 4. Yoo CS, Kim YM, Kim HY. Impact of chronic kidney disease on depression, perceived health, and health-related quality of life: Results from the Korea National Health and Nutrition Examination Survey in 2014 and 2016. Korean Journal of Adult Nursing. 2020;32(4):374–384. https://doi.org/10.7475/kjan.2020.32.4.374Article
- 5. Ko HL, Min HK, Lee SW. Self-rated health and the risk of incident chronic kidney disease: A community-based Korean study. Journal of Nephrology. 2023;36(3):745–753. https://doi.org/10.1007/s40620-022-01518-3ArticlePubMed
- 6. Grove BE, Schougaard LM, Hjollund NH, Ivarsen P. Self-rated health, quality of life and appetite as predictors of initiation of dialysis and mortality in patients with chronic kidney disease stages 4-5: A prospective cohort study. BMC Research Notes. 2018;11(1):371. https://doi.org/10.1186/s13104-018-3472-9ArticlePubMedPMC
- 7. Lee J, Abdel-Kader K, Yabes JG, Cai M, Chang HH, Jhamb M. Association of self-rated health with functional limitations in patients with CKD. Kidney Medicine. 2021;3(5):745–752. https://doi.org/10.1016/j.xkme.2021.04.010ArticlePubMedPMC
- 8. Baddour NA, Robinson-Cohen C, Lipworth L, Bian A, Stewart TG, Jhamb M, et al. The surprise question and self-rated health are useful screens for frailty and disability in older adults with chronic kidney disease. Journal of Palliative Medicine. 2019;22(12):1522–1529. https://doi.org/10.1089/jpm.2019.0054ArticlePubMedPMC
- 9. Yoo HJ, Ahn SH. Influences of health-related information-seeking behavior, the health locus of control, and sense of coherence on self-rated health in South Korean patients with colorectal cancer. Global Health and Nursing. 2019;9(2):48–59. https://doi.org/10.35144/ghn.2019.9.2.48Article
- 10. Nayak S, Nayak SR, Alice A, Sahoo D, Kanungo S, Rehman T, et al. Factors associated with poor self-rated health among chronic kidney disease patients and their health care utilization: Insights from LASI wave-1, 2017-18. Frontiers in Nephrology. 2023;2:968285. http://doi.org/10.3389/fneph.2022.968285ArticlePubMedPMC
- 11. Robinson-Cohen C, Hall YN, Katz R, Rivara MB, de Boer IH, Kestenbaum BR, et al. Self-rated health and adverse events in CKD. Clinical Journal of the American Society of Nephrology. 2014;9(12):2044–2051. https://doi.org/10.2215/cjn.03140314ArticlePubMedPMC
- 12. Jafari M, Kour K, Giebel S, Omisore I, Prasad B. The burden of frailty on mood, cognition, quality of life, and level of independence in patients on hemodialysis: Regina hemodialysis frailty study. Canadian Journal of Kidney Health and Disease. 2020;7:2054358120917780. https://doi.org/10.1177/2054358120917780ArticlePubMedPMC
- 13. Wen J, Jin X, Al Sayah F, Short H, Ohinmaa A, Davison SN, et al. Mapping the edmonton symptom assessment system-revised: Renal to the EQ-5D-5L in patients with chronic kidney disease. Quality of Life Research. 2022;31(2):567–577. https://doi.org/10.1007/s11136-021-02948-5ArticlePubMed
- 14. Hong JH. Relative importance of the EQ-5D five dimensions among patients with chronic diseases in South Korea – a comparison with the general population preference weights. Health and Quality of Life Outcomes. 2018;16(1):1–10. http://doi.org/10.1186/s12955-018-0987-7ArticlePubMedPMC
- 15. Lee CE, Chun DI. The relationship between subjective health perception, depression, and quality of life in stroke patients: Focusing on the regulated mediating effect of stress. Kookmin Social Science Reviews. 2022;35(1):59–82. https://doi.org/10.54711/KSSR.35.1.03Article
- 16. Lee KE, Cho EH. Factors influencing health related quality of life in patients with hypertension: Based on the 5th Korean National Health and Nutrition Examination Survey. The Journal of the Korea Contents Association. 2016;16(5):399–409. http://doi.org/10.5392/JKCA.2016.16.05.399Article
- 17. Kim SH, Kim MO. Factors affecting health-related quality of life in patients with chronic obstructive pulmonary disease using health-related quality of life instrument with 8 Items. The Journal of the Korea Contents Association. 2022;22(8):347–357. https://doi.org/10.5392/JKCA.2022.22.08.347Article
- 18. Jee YJ, Park YS. Factors influencing the quality of life of diabetics. Asia-pacific Journal of Multimedia Services Convergent with Art, Humanities, and Sociology. 2019;9(10):459–467. http://doi.org/10.35873/ajmahs.2019.9.10.039Article
- 19. Legrand K, Speyer E, Stengel B, Frimat L, Ngueyon Sime W, Massy ZA, et al. Perceived health and quality of life in patients with CKD, including those with kidney failure: Findings from national surveys in France. American Journal of Kidney Diseases : The Official Journal of the National Kidney Foundation. 2020;75(6):868–878. .https://doi.org/10.1053/j.ajkd.2019.08.026ArticlePubMed
- 20. Korean Centers for Disease Control and Prevention. The 8th Korea national health and nutrition examination survey (2016- 2018) [Internet]. Seoul: Korean Centers for Disease Control and Prevention. 2020 [cited 2023 Apr 22]. Available from: https://knhanes.kdca.go.kr/knhanes/sub03/sub03_02_05.do
- 21. Korea Health Promotion Institute. Low-risk drinking guidelines [Internet]. Seoul: Korea Health Promotion Foundation. 2013 [cited 2023 Apr 26]. Available from: https://www.khepi.or.kr/fileDownload?titleId=23674&fileId=2&fileDownType=%27C%27
- 22. Cullati S, Bochatay N, Rossier C, Guessous I, Burton-Jeangros C, Courvoisier DS. Does the single-item self-rated health measure the same thing across different wordings? Construct validity study. Quality of Life Research : An International Journal of Quality of Life Aspects of Treatment, Care and Rehabilitation. 2020;29(9):2593–2604. https://doi.org/10.1007/s11136-020-02533-2ArticlePubMedPMC
- 23. Ambagtsheer RC, Visvanathan R, Dent E, Yu S, Schultz TJ, Beilby J. Commonly used screening instruments to identify frailty among community-dwelling older people in a general practice (primary care) setting: A study of diagnostic test accuracy. The Journals of Gerontology. Series A. 2020;75(6):1134–1142. https://doi.org/10.1093/gerona/glz260Article
- 24. Limin L, Chaojie L, Xiuzhi C, Hongjuan Y, Xueyun Z, Mingjie S, et al. Validity and reliability of the EQ-5D-5 L in family caregivers of leukemia patients. BMC Cancer. 2019;19:522. https://doi.org/10.1186/s12885-019-5721-2Article
- 25. Abedini MR, Bijari B, Miri Z, Shakhs Emampour F, Abbasi A. The quality of life of the patients with diabetes type 2 using EQ-5D-5 L in Birjand. Health and Quality of Life Outcomes. 2020;18(1):1–9. https://doi.org/10.1186/s12955-020-1277-8ArticlePubMedPMC
- 26. Willerth M, Ahmed T, Phillips SP, Pérez-Zepeda MU, Zunzunegui MV, Auais M. The relationship between gender roles and self-rated health: A perspective from an international study. Archives of Gerontology and Geriatrics. 2020;87:103994. https://doi.org/10.1016/j.archger.2019.103994ArticlePubMed
- 27. Ge L, Ong R, Yap CW, Heng BH. Effects of chronic diseases on health-related quality of life and self-rated health among three adult age groups. Nursing and Health Sciences. 2019;21(2):214–222. https://doi.org/10.1111/nhs.12585ArticlePubMed
- 28. Yoo YJ. The mediating role of smoking and body mass index on the relationship between alcohol consumption and blood triglyceride levels among Korean adults: The 7th Korean National Health and Nutrition Examination Survey. Korean Journal of Health Promotion. 2021;21(4):167–174. https://doi.org/10.15384/kjhp.2021.21.4.167Article
- 29. Zhang Y, Li J, Yang L. Health-related quality of life of Chinese patients with chronic kidney disease: A study based on four EQ-5D-3L value sets. Scientific Reports. 2023;13(1):7863. https://doi.org/10.1038/s41598-023-35002-0ArticlePubMedPMC
 PubReader
PubReader ePub Link
ePub Link Cite
Cite