Articles
- Page Path
- HOME > Res Community Public Health Nurs > Volume 35(1); 2024 > Article
-
Original Article
- Home-based walking intervention for middle-aged migrant women using 360-degree virtual videos and a wearable activity tracker: A mixed-methods pilot study
-
Duckhee Chae1
 , Keiko Asami2, Jaseon Kim3, Kukhyeon Kim4, Jeeheon Ryu5, Ardith Z. Doorenbos6
, Keiko Asami2, Jaseon Kim3, Kukhyeon Kim4, Jeeheon Ryu5, Ardith Z. Doorenbos6 -
Research in Community and Public Health Nursing 2024;35(1):10-21.
DOI: https://doi.org/10.12799/rcphn.2023.00339
Published online: March 29, 2024
1Professor, College of Nursing, Chonnam National University, Gwangju, Korea
2Doctoral student, College of Nursing, Chonnam National University, Gwangju, Korea
3Assistant professor, Department of Nursing, Nambu University, Gwangju, Korea
4Instuctor, Department of Education, Chonnam National University, Gwangju, Korea
5Professor, Department of Education, Chonnam National University, Gwangju, Korea
6Professor, Department of Biobehavioral Nursing Science, College of Nursing, University of Illinois, Chicago, Illinois, USA
- Corresponding author: Keiko Asami College of Nursing, Chonnam National University, 160 Baekseo-ro, Dong-gu, Gwangju 61469, Korea Tel: +82-62-530-4942, Fax: +82-62-220-4544, E-mail: asami1121@hanmail.net
© 2024 Korean Academy of Community Health Nursing
This is an Open Access article distributed under the terms of the Creative Commons Attribution NoDerivs License. (http://creativecommons.org/licenses/by-nd/4.0) which allows readers to disseminate and reuse the article, as well as share and reuse the scientific material. It does not permit the creation of derivative works without specific permission.
- 1,868 Views
- 25 Download
Abstract
-
Purpose
- To sustain behavior change, an intervention strategy that considers the contribution of affect to daily physical activity behavior regulation is needed. Although virtual reality-based physical activity interventions have the potential to improve emotional status, interventions using virtual reality videos in a free-living environment are lacking. This pilot study assessed the feasibility and preliminary efficacy of a home-based intervention using 360-degree virtual videos and wearable activity trackers to improve mood and physical activity.
-
Methods
- A one-group pilot study of 12 middle-aged migrant women asked participants to watch virtual reality videos and perform moderate-intensity walking 5 days per week for 4 weeks, then complete surveys and focus group interviews. The intervention’s feasibility and preliminary efficacy were assessed by examining recruitment, retention, adherence, acceptability, mood, physical activity, and exercise self-efficacy.
-
Results
- A word-of-mouth approach was effective for recruiting participants. Although the weekly intervention adherence rate ranged from 53.5% to 83.5%, retention (92.3%) and acceptability (91.7%) were high. Participants were satisfied with the “visual status indicators,” “sense of accomplishment and confidence,” “emotional engagement and sense of presence,” “joy from exercise,” “external motivation through supervision,” “easy to control virtual reality device,” and “extra benefits” of the intervention. Participants had significant decreases in negative affect (p=.016). Positive affect, physical activity, and exercise self-efficacy showed trends toward improvement.
-
Conclusion
- This home-based intervention employing virtual reality videos and Fitbit activity trackers is feasible and shows preliminary efficacy in improving mood. Further research is warranted to evaluate its effectiveness in a more rigorous randomized controlled trial.
- 1. Background
- The health benefits of physical activity, including improved mental health and quality of life, are well established [1]. Yet globally, more than a quarter of all adults do not participate in enough physical activity [2]. The Korea National Health and Nutrition Examination Survey results reported that regular participation in aerobic physical activity among Korean adults has tended to decline over time. Regular participation in physical activity is highest in people’s 20s and declines with age, and women tend to engage in less physical activity than men [3]. Both physical inactivity and depressive symptoms have been found to be common in migrants 50 years and older [4,5]. For instance, a recent study reported that only 15.8% of middle-aged Japanese migrant women in Korea engaged in regular physical activity [6].
- Many studies have examined the relationship between physical activity and affective responses. Overall, these studies have shown that physical activity influences positive affect [7,8]. However, in the physical activity–affect relationship, physical activity not only elicits an affective response but affect also regulates physical activity behavior. Specifically, positive affect increases physical activity, while negative affect decreases physical activity [9]. Therefore, to sustain long-term behavior change, an intervention strategy that considers the contribution of affect to daily physical activity behavior regulation is needed. Using immersive technology such as virtual reality (VR) as part of a physical activity intervention strategy could serve this purpose.
- Providing an immersive experience could be a crucial element of physical activity interventions for physically inactive people. Immersive experiences can facilitate authentic engagement in stimulating the senses and emotions [10]. Such immersive experiences bring delightful psychological states to individuals who are deeply participating [11-14]. VR is a way to produce such immersive engagement for physical activity interventions [15,16]. VR-based environments create intensive immersion, in which users are engaged in and involved with desirable emotional states.
- In recent studies, VR use has been found to improve emotional well-being [11,12,14]. For example, VR videos of nature improved positive affect by helping middle-aged women with depression feel connected to nature [14]. And among older adults, 360-degree video-based VR produced enjoyable experiences with low levels of physical and emotional discomfort [11]. However, VR-based health care studies have mainly focused on rehabilitation and physical function and mainly involved one-time experiments in laboratories with researchers supervising or assisting [17-20]. Although VR-based physical activity interventions have great potential to improve people’s emotional status, studies of the usability and acceptability of VR video-based interventions in community settings are lacking [19]. One of the primary motivations for the present study is to address interventions for physical activity behavior change using VR videos in a free-living environment.
- Due to limited previous studies on physical activity behavior change using VR videos in a free-living environment, a small-scale test of methods and procedures to assess the feasibility of the intervention before a large-scale study is an important step in the development phase [21]. This offers insight into the advantages or disadvantages, practicability, or any modifications needed in the research methods or protocols. The purpose of this pilot test was to assess the feasibility and preliminary efficacy of a home-based intervention for middle-aged migrant women that employed VR videos and wearable activity trackers.
- 2. Theoretical Framework
- Based on recent studies [22,23] examining the feasibility of innovative 4-week digital device-based interventions to promote physical activity, we developed a 4-week home-based intervention called Create a Healthy Lifestyle Routine. Self-efficacy has been reported as a major psychosocial mechanism with positive effects on initiating and maintaining physical activity [24,25], and this intervention was developed to address the four main sources of self-efficacy identified by Bandura: mastery experience, vicarious experience, verbal persuasion, and emotional arousal [26]. The intervention included a wearable activity tracker, weekly summary report, goal-setting consultation, logbook (for mastery experience), short animation video (for vicarious experience), text messages (for verbal persuasion), and 360-degree VR nature videos (for emotional arousal). Because knowledge of health risks and the benefits of health practices is a precondition for change [27], a 30-minute in-person education session was also provided (Table 1, Figure 1).
Introduction
- 1. Study Design
- This mixed-methods pilot test employed a quantitative one-group pre-posttest design and qualitative focus group interviews.
- 2. Setting and Sample
- The study was conducted between April and July 2021 in Gwangju and Jeollanam Provinces of South Korea. Potential participants were recruited from five churches, which were attended predominantly by Japanese migrant women. A Japanese research staff member contacted leaders of the five churches to obtain their permission to conduct recruitment activities and to request contact information for church members. Then a recruitment letter with a hyperlink to an online screening survey (Google Surveys) was sent to potential participants through social networking service (SNS) and text messages. Migrant women who had an interest in participating were asked to respond to the online screening survey.
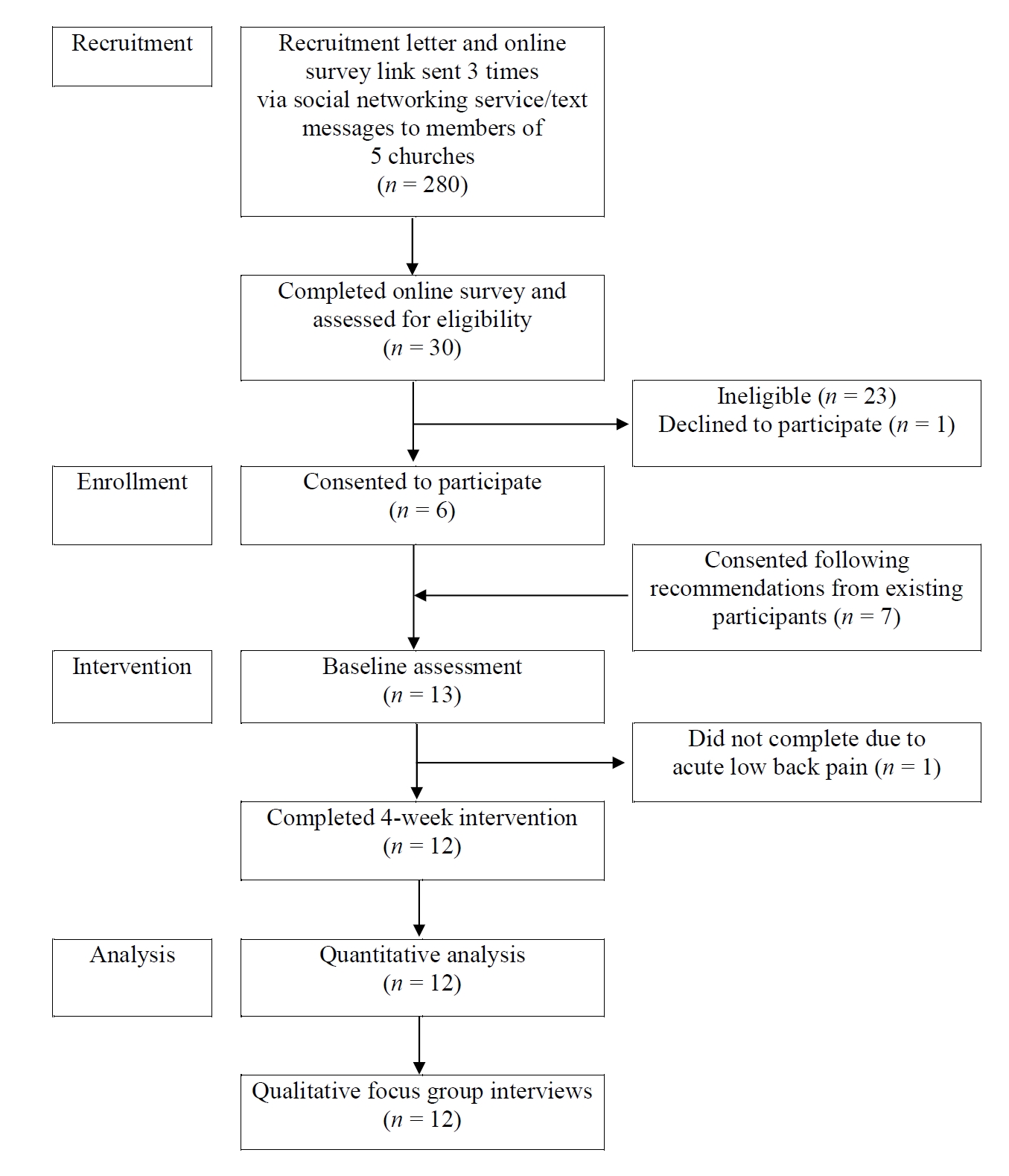
- Under the study inclusion criteria, participants had to be women aged 40 to 64 years, be a migrant in Korea, use a smartphone and Wi-Fi at home, not be engaging in regular exercise (i.e., at least 150 minutes of moderate-to-vigorous physical activity [MVPA] weekly), not have any illnesses that would prevent walking and VR use, not be currently enrolled in any other exercise program, and speak and understand Korean. Research staff confirmed the eligibility of each prospective participant by telephone and then scheduled an in-person meeting. Four cohorts of 3–4 participants each were recruited sequentially, with a total of 13 migrant women who consented to participate in the pilot test. One individual did not complete the intervention due to back pain, thus we analyzed data for the 12 participants who completed the intervention (Figure 2).
- 3. Intervention
- One week before the beginning of the intervention, participants were provided with a Fitbit Charge 3 (Fitbit Inc, San Francisco, CA, USA) with an education on the Fitbit device and asked to wear it during their walking hours for 7 days. The following week, research staff provided the 30-minute in-person education on physical activity and body composition, and participants practiced head-mounted display use and completed a baseline assessment. Then participants set their individual physical activity goals in consultation with research staff. During the 4-week intervention period, participants were asked to watch VR videos for 5–10 minutes at least 5 days per week and perform moderate-intensity walking for at least 30 minutes at least 5 days per week. For the VR videos, the research staff initially selected a pool of 14 360-degree VR nature videos of less than 5 minutes’ duration from YouTube. Next, a psychologist rated how appropriate each of the 14 videos was for improving emotional well-being on a 4-point scale (1=not appropriate, 2=somewhat appropriate, 3=quite appropriate, and 4=very appropriate). Twelve videos rated 3 or 4 were used for the intervention.
- 4. Data Collection
- Quantitative data were collected using surveys administered at baseline and at 4 weeks, immediately post-intervention. Qualitative data were collected through 30- to 60-minute focus group interviews conducted after participants completed the post-intervention survey. The interviews started with questions such as “What changes did you feel while participating in the program?” and “How was your experience using VR device and Fitbit?” All interviews were conducted by the first author, who has extensive experience in migrant healthcare, using a semi-structured interview guide. All interviews were audiotaped and were immediately transcribed and analyzed.
- 5. Measures
- The primary outcome of this study was feasibility, which was assessed using recruitment rate, retention rate, adherence rate, and acceptability. Recruitment rate, which assesses the feasibility of recruiting a sufficient number of participants for the study [28], was measured as the number of individuals agreeing to participate divided by the number of potential participants screened. Retention rate, which assesses the ability to maintain an adequate proportion of participants [28], was measured as the number of participants completing the 4-week post-intervention survey divided by the 13 initial participants. Adherence rate, which assesses the degree to which participants adhere to intervention protocols [28], was measured as the number of participants who completed the home-based intervention (based on the VR viewing log recorded by participants and the exercise time recorded by the Fitbit) divided by 12 participants. Acceptability, which assesses the extent to which the intervention is acceptable to intervention recipients [28], was measured using a single question, “How satisfied are you with this program overall?” with a 5-point response scale (ranging from 1=very dissatisfied to 5=very satisfied). Acceptability was further explored through focus group interview questions about participants’ experiences with using the Fitbit and VR videos as well as their approval and/or disapproval of components of the intervention.
- The secondary outcome of this study was preliminary efficacy, which was assessed using mood, physical activity, and exercise self-efficacy. Among these, mood and exercise self-efficacy were measured using self-report questionnaires. To reduce measurement errors that may arise due to language and cultural differences, we used Japanese versions of instruments that were psychometrically validated for Japanese adults [29,30].
- Mood was measured using the 22-item Japanese Positive and Negative Affect Schedule (11 items each for positive and negative affect) [29]. Responses were scored on a 5-point scale (ranging from 1=felt very slightly or not at all to 5=felt very much), with a higher score indicating a stronger corresponding emotion. The Cronbach’s alpha in the present study was .92–.95 for positive affect and .84–.89 for negative affect.
- Physical activity was measured by the daily time MVPA at ≥3 metabolic equivalents and daily step count recorded on each participant’s Fitbit Charge 3. Participants were instructed to put the device on every morning at the start of the day’s activity and take it off in the evening at the end of the day’s activity.
- Exercise self-efficacy was measured using the 5-item Japanese Self-Efficacy for Exercise scale [30], which measures belief in one’s ability to perform exercise regularly. Responses were scored on a 5-point scale (ranging from 1=strongly disagree to 5=strongly agree), with a higher score indicating a stronger corresponding self-efficacy. The Cronbach’s alpha in the present study was .70–.79.
- 6. Data Analysis
- The quantitative data were analyzed using IBM SPSS v.23.0 with the significance level α=.05. Paired t-tests and Wilcoxon signed-rank tests were conducted to examine participants’ mood, physical activity, and exercise self-efficacy between baseline and week 4. In addition, standardized effect size measures were calculated. In an attempt to correct for the small sample size, the Hedges’ g effect size and its 95% confidence interval were employed [31].
- Inductive content analysis was used to analyze the qualitative data [32]. From the interview transcriptions, units of meaning (words, sentences) describing acceptability were identified and condensed into descriptive texts. Then, the data were categorized by combining statements that belonged together. Subsequently, these consolidated statements were further combined into two categories: advantages of the intervention and areas needing improvement. The three authors analyzed these texts through repeated discussions concerning interpretations and categorizations until consensus was attained.
- 7. Ethical Considerations
- This study was approved by the institutional review board of Chonnam National University (No. 1040198-200720-HR-078-04). Information concerning the purpose of the study, participant anonymity, and voluntary participation was provided to all participants, and written, informed consent was obtained from all participants. All materials provided to participants were written in Japanese. The education sessions and qualitative focus group interviews were conducted in a mixture of Japanese and Korean. During the study period, we prioritized the protection of participants according to local COVID-19 prevention and quarantine procedures. All participants received US$25 in remuneration after completing each of the baseline and final assessment visits (for a total of US$50).
Methods
1) Primary outcomes: Feasibility
2) Secondary outcomes: Preliminary efficacy
- 1. Study Participants
- The participants’ mean age was 54.23 (SD=4.43) years, and their mean years of living in Korea was 23.56 (SD=3.46). All had a high-school diploma or had completed a higher level of education. Most (83.3%) were married and employed. The majority (66.6%) had a monthly household income of less than 3 million Korean won (Supplemental Table 1).
- 2. Feasibility
- Study recruitment letters were sent to a total of 280 Japanese migrant women. We assessed interest and study eligibility in 30 women who responded to the recruitment letter. Of those, one woman who was eligible declined to participate and 23 women were found ineligible because of health conditions, regular exercise, or no contact information. In addition, seven migrant women agreed to participated in the study at the recommendation of the six initial participants (Figure 2). In total, 37 potential participants were screened over 14 weeks, of which 13 agreed to participate, resulting in a recruitment rate of 35.1%.
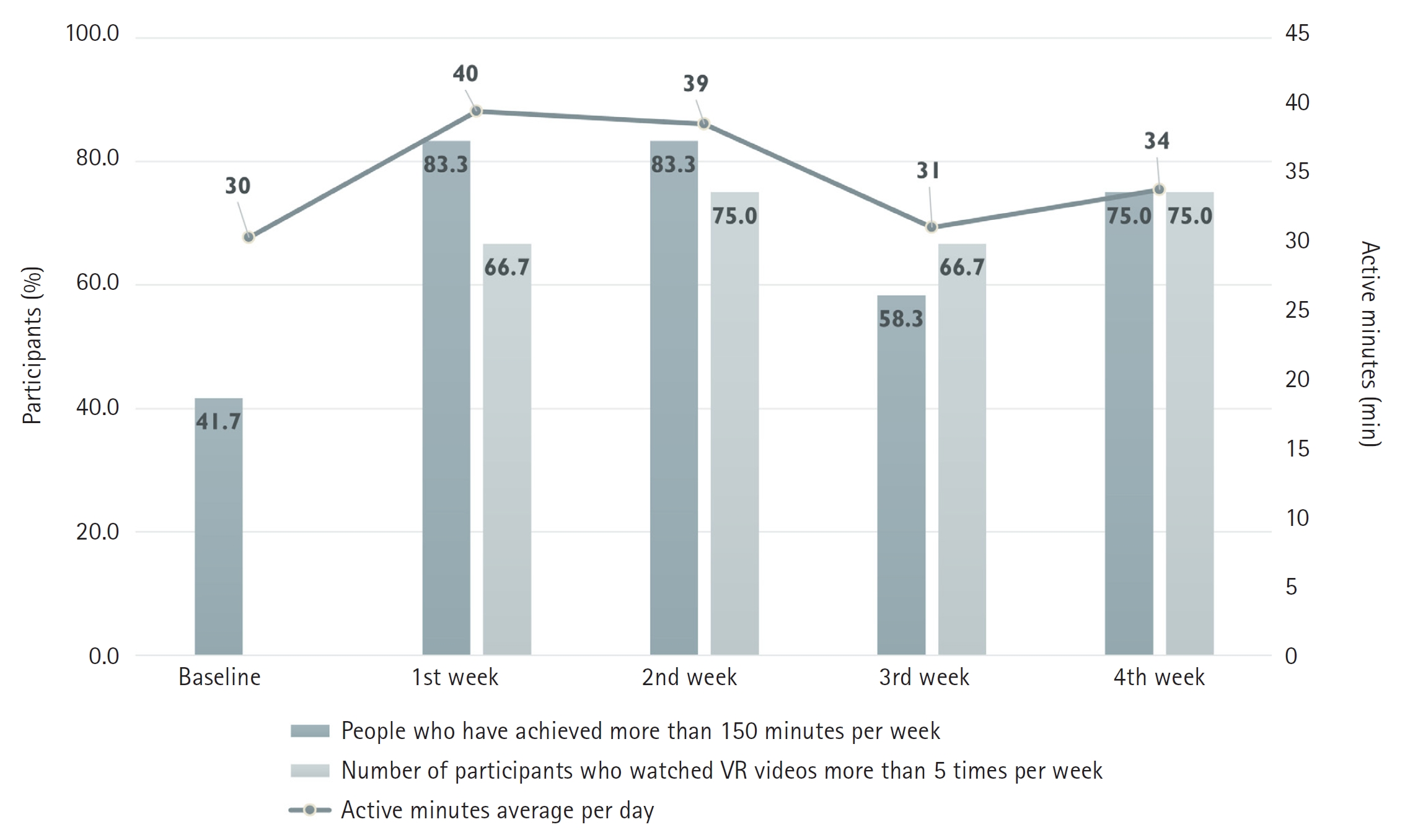
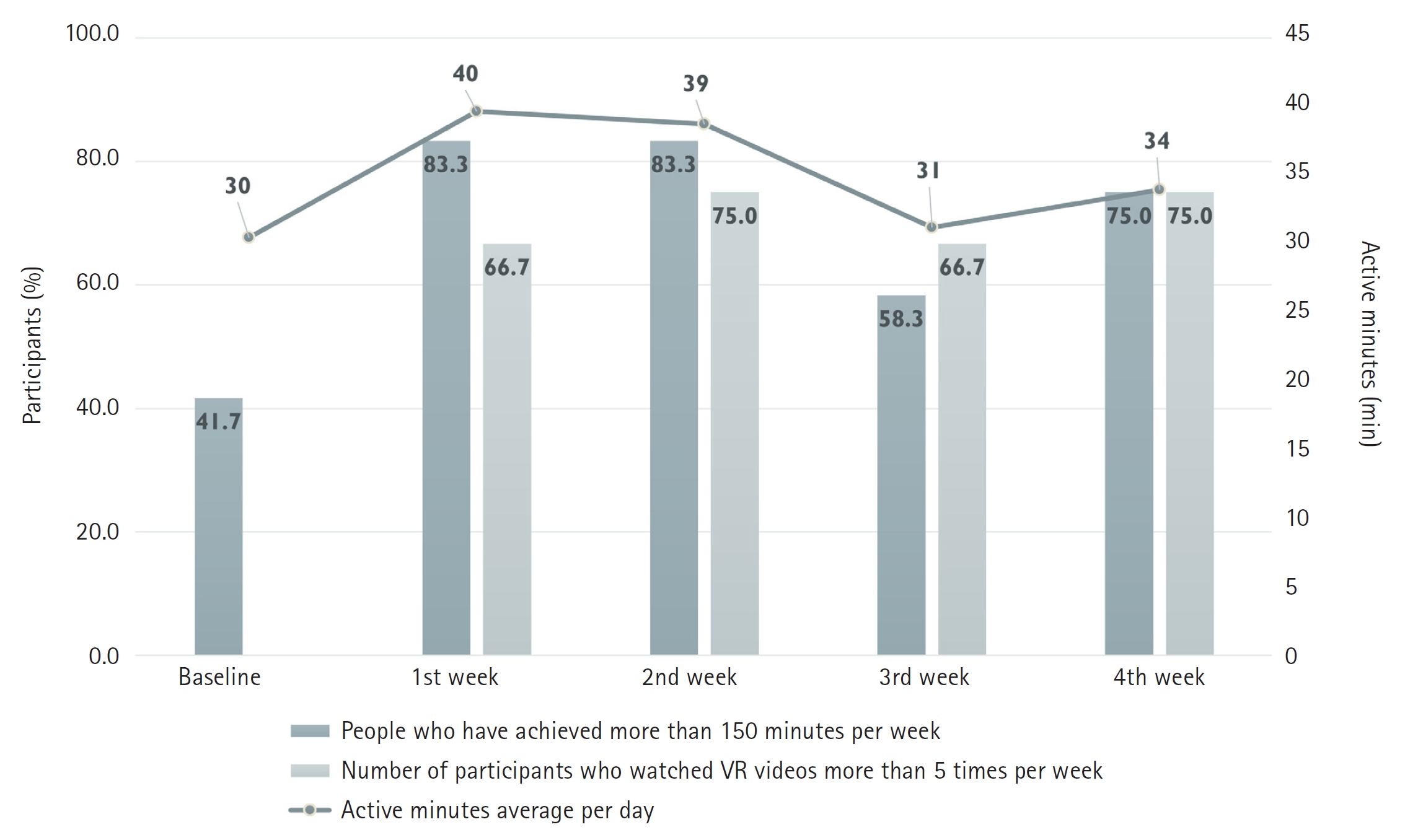
- During the 4-week intervention, one of the 13 initial participants stopped participating in the intervention due to back pain, resulting in a retention rate of 92.3%. The adherence rate for watching the VR videos was 66.7% in the first week, 75.0% in the second week, 66.7% in the third week, and 75.0% in the fourth week. Participants mostly watched the videos between 5 and 7 a.m. and 6 and 11 p.m. The adherence rate for moderate-intensity physical activity was 83.3% in the first and second weeks, 58.3% in the third week, and 75.0% in the fourth week (Figure 3). Acceptability was high, with 91.7% of participants saying they were “satisfied” or “very satisfied” with the overall intervention (mean=4.08 out of 5.00).
- Participants’ comments regarding satisfaction with the intervention and areas requiring improvement are summarized in Supplemental Table 2. The “visual status indicators” provided by the Fitbit encouraged the participants to achieve their daily exercise goals, and through this process, participants felt a “sense of accomplishment and confidence.” The VR videos increased participants’ “emotional engagement and sense of presence.” The “easy-to-control VR device” allowed the participants to watch videos without difficulty in their homes. The text messages provided participants with “external motivation through supervision.” Participants experienced not only “joy from exercise” but also the “extra benefits” of being able to talk with their children while walking and get a good night’s sleep. The areas of the intervention that required improvement included “discomfort caused by equipment,” “video content diversity,” and “additional intervention elements.”
- 3. Preliminary Efficacy
- The results of paired t-test analyses indicated that only negative affect was significantly changed (reduced) after the intervention (p=.016). Changes in physical activity, positive affect, and exercise self-efficacy showed trends, but did not reach statistical significance. The Hedges’ g standardized mean difference effect size was 0.72 (95% CI=0.09, 1.43) for changes in self-efficacy and -0.52 (95% CI=-0.99, -0.10) for changes in negative affect (Table 2).
Results
- 1. Feasibility
- The ability to effectively recruit participants in a timely manner is a key determinant of an intervention’s ultimate success [33]. In this study, a culturally matched research staff member recruited participants from church-based community networks using passive (SNS and text messages) and active (word-of-mouth) approaches. Many walking studies use more than one recruitment approach [33,34]. Compared to word-of-mouth, the SNS and text messages reached a larger number of migrant women; however, the expected yield of eligible participants was lower with passive messaging (20% recruited) than with word-of-mouth (100% recruited). These results are similar to those of Gilliss and colleagues [35] in their community-based study of healthy ethnic minority women, where face-to-face recruiting yielded the highest percentage of eligible participants (74%), and internet website recruiting yielded the lowest (21%). Interestingly, in our study, all migrant women recruited via word-of-mouth had already known about the intervention from our recruitment letter but had postponed their participation until they received positive opinions on the intervention from an acquaintance. Therefore, when planning health interventions for migrant women, it is crucial to identify the role of opinion leaders in advance, identify opinion leaders using multiple methods, and then involve them in the recruitment stage [36].
- In this study, the weekly intervention adherence rates were 66.7% to 75.0% for VR videos and 58.3% to 83.3% for MVPA. To maintain motivation for behavior change, additional strategies seem necessary after the initial 2-3 weeks of the intervention. More specifically, the adherence rate for MVPA among our study participants maintained at 83.3% during the initial two weeks, then dropped to 58.3% in the third week, but tended to rise again (75.0%) in the fourth week. Nyenhuis et al. [37] conducted a 7-week walking intervention for urban African American women, with similar intervention elements as this study (e.g., self-monitoring with Fitbit, goal setting, group sessions, and text messages) besides VR videos. While adherence to step goals reached 71.4-72.6% in the initial weeks, it dropped to 55.1% in week four and remained within 51.0-60.5% until the end, showing no significant recovery. Understanding whether VR intervention can mitigate the rebound in adherence to physical activity requires a randomized controlled trial.
- In the case of the VR videos, the limited video selection options appear to have influenced adherence. Half the videos used in this study depicted underwater scenes, and some participants had unpleasant memories or fears of water, so their options were even more limited, and their interest decreased over time. A user-friendly virtual environment has a greater effect on the user’s emotions than a general virtual environment and thus improves immersion [18]. In fact, some participants wanted to see VR videos showing the scenery of their hometown or of famous tourist destinations. In this study, we provided links to YouTube VR videos; by doing this, we avoided content production costs, but it was not possible to provide customized content reflecting participant preferences.
- Most of the participants (91.7%) were satisfied or very satisfied with the intervention. Wearable devices are known to serve as a facilitator in motivating and accelerating physical activity [38], and in our focus group interviews, study participants reported similar experiences with this study’s head-mounted display and Fitbit. In planning the intervention, we considered engaging middle-aged migrant women in an intervention involving a new technology to be the greatest challenge. However, we found that participant acceptance of the VR videos was good, and no adverse events were reported. We conclude that, with 20 minutes of practice, middle-aged migrant women can enjoy VR videos on their own at home while wearing an immersive headset. This suggests that VR technology has strong potential for use in home-based interventions.
- 2. Preliminary Efficacy
- This study demonstrated that a home-based intervention combining a Fitbit and VR videos has the potential to improve emotional well-being and exercise self-efficacy in middle-aged migrant women. In particular, the intervention showed preliminary efficacy at reducing negative affect. This finding differs from some previous studies in which physical activity improved positive affect but did not decrease negative affect [7,8]. On the other hand, when Browning et al. [39] tested the effects of outdoor nature exposure and 360-degree VR nature videos on mood, negative affect was significantly decreased by both outdoor nature exposure and the VR nature videos, whereas positive affect showed a significant change only with outdoor nature exposure. Therefore, we assume that the emotional engagement our participants reported experiencing while viewing the 360-degree VR videos, such as stability, comfort, and freedom, may have contributed to decreased negative affect. However, given our one-group study design, it is not possible to determine whether the decrease in negative affect was due to physical activity, the VR videos, or the intervention as a whole.
- All the participants initially described themselves as inactive, but during their baseline assessments with the Fitbit, we found that their average daily MVPA time was 30 minutes or more, indicating that they were already achieving an acceptable level of physical activity. This finding may be due to their domestic and work-related physical activities, as most participants cared for families and were employed. In addition, women who are mainly engaged in manual labor at work tend to be more physically inactive in their leisure time [40]. Our study participants were usually inactive during their leisure time, but during the intervention, they reported experiencing joy after exercise and feeling intrinsic and extrinsic motivation to exercise. Although a 4-week home-based intervention may not be sufficient to create a physical activity habit, our observations of increases in exercise self-efficacy and decreases in negative affect indicate the potential benefits of the intervention. Further studies are needed to evaluate the efficacy of the intervention on the enhancement of leisure time physical activity in migrant women.
- During the focus group interviews, participants identified areas of the intervention that need improvement. First, participants indicated that some face-to-face sessions would be desirable. As adding human support is known to promote engagement with many interventions [41], it is not surprising that migrant women reported wanting some face-to-face time. However, a face-to-face behavior change intervention requires participants to attend a set number of scheduled sessions, whereas a digital behavior change intervention can engage individuals whenever they are available [42]. Moreover, programs and devices using digital technology have been shown to improve health by supporting healthy behaviors [42-45]. In any case, because providing our intervention face-to-face would increase the cost, it would be necessary to devise a strategy for cost-effectively providing some face-to-face sessions [42].
- As two other areas for improvement, participants suggested increasing the diversity of content in the VR videos and taking measures to reduce the discomfort caused by the wearable devices. Regarding the second suggestion, device-measured physical activity has the advantage of producing more reliable and valid results. However, some participants reported that they often forgot to wear the Fitbit, so their physical activity were not accurately measured. Thus, there is a possibility that a statistically significant change in their physical activity was not captured in the study. We did use in-person education and an animation video to encourage regular Fitbit wear, but these were insufficient. The same problem was reported in a previous study conducted to promote physical activity in migrant women [46]. To obtain accurate measurements of physical activity levels, additional strategies such as physical activity logs and text message reminders are needed to promote adherence to protocols for wearable activity trackers.
Discussion
- This study had a few limitations. Given its one-group design, this study poses limitations in establishing causal relationships and is susceptible to the influence of confounding factors [47]. Moreover, it was not possible to determine which components of the intervention (VR videos or activity trackers or both) affected participants’ mood changes. Utilizing a randomized controlled trial design will enhance the validity and interpretation of the study outcomes. Another limitation is that the small sample size raises the risk of a Type II error, potentially hindering the statistical significance detection of the intervention effect. In addition, the number and content of the VR videos used for the intervention were limited, and the participants’ preferences were not known during video selection. This may have affected the efficacy of the VR video use for improving emotional well-being and physical activity. The study participants were Japanese women who had lived in Korea for an average of 23.56 years, all holding at least a high school diploma. Furthermore, considering the low recruitment rate of 35.1%, individuals participating in this study may also possess characteristics suggestive of a willingness to adopt new technologies and devices, such as VR or Fitbit. Therefore, there are limitations in generalizing the results of this study to other immigrant women. Finally, physical activity was consistently assessed in participants' natural settings utilizing Fitbit, while moods were assessed using a self-reported questionnaire in a paper-and-pencil mode once before and after the intervention. In future research, it is recommended to employ ecological momentary assessment, which involves repeated real-time assessments of participants’ mood in their natural environments [48]. This will better help understand how interventions experienced in real life impact mood changes.
Limitation
- This study’s home-based intervention, employing VR videos and wearable activity trackers, is feasible in terms of high retention and acceptability. To maximize recruitment of middle-aged migrant women, multiple recruitment approaches, including word-of-mouth, are needed. To increase the intervention adherence rate, additional strategies are needed, including diversifying VR video content and providing face-to-face intervention sessions with appropriate frequency. The intervention shows preliminary efficacy in improving mood, especially negative affect. Further research is warranted to evaluate the intervention’s effectiveness in a more rigorous randomized controlled trial.
Conclusions
SUPPLEMENTARY MATERIALS
Supplementary Table 1.
Supplementary Table 2.
-
Conflict of interest
Duckhee Chae has been editorial board member of the Research in Community and Public Health Nursing. She was not involved in the review process of this manuscript. No conflict of interest has been declared by all authors.
-
Funding
This work was supported by the Ministry of Education of the Republic of Korea and the National Research Foundation of Korea (NRF-2021S1A5C2A02089141). The funder did not play any role in the conduct or publication of the study.
-
Authors’ contributions
Duckhee Chae contributed to conceptualization, data curation, formal analysis, funding acquisition, methodology, project administration, visualization, writing - original draft, review & editing, investigation, resources, supervision, and validation. Keiko Asami, Jaseon Kim, and Kukhyeon Kim contributed to conceptualization, data curation, formal analysis, methodology, project administration, visualization, writing - original draft, review & editing, investigation, resources, and software. Jeeheon Ryu contributed to conceptualization, data curation, methodology, project administration, writing - review&editing, supervision, and validation.
Ardith Z. Doorenbos contributed to writing - review&editing, supervision, and validation.
-
Data availability
Please contact the corresponding author for data availability.
NOTES
Acknowledgments


- 1. 2018 Physical Activity Guidelines Advisory Committee. 2018 Physical activity guidelines advisory committee scientific report [Internet]. Washington: Office of the Assistant Secretary for Health; 2018 [cited 2018 Feb 1]. Available from https://health.gov/sites/default/files/2019-09/PAG_Advisory_Committee_Report.pdf
- 2. Guthold R, Stevens GA, Riley LM, Bull FC. Worldwide trends in insufficient physical activity from 2001 to 2016: A pooled analysis of 358 population-based surveys with 1·9 million participants. The Lancet Global Health. 2018;6(10):e1077–e1086. https://doi.org/10.1016/S2214-109X(18)30357-7ArticlePubMed
- 3. Korea Disease Control and Prevention Agency. Physical activity [Internet]. Cheongju: Korea Disease Control and Prevention Agency. 2022 [Cited 2023 Jan 23]. Available from https://knhanes.kdca.go.kr/knhanes/sub01/sub01_05.do#header
- 4. Aichberger MC, Schouler-Ocak M, Mundt A, Busch MA, Nickels E, Heimann HM, et al. Depression in middle-aged and older first generation migrants in Europe: Results from the Survey of Health, Ageing and Retirement in Europe (SHARE). Europian. 2010;25(8):468–475. https://doi.org/10.1016/j.eurpsy.2009.11.009ArticlePubMed
- 5. Kristiansen M, Razum O, Tezcan-Güntekin H, Krasnik A. Aging and health among migrants in a European perspective. Public Health Reviews. 2016;37(1):1–14. https://doi.org/10.1186/s40985-016-0036-1ArticlePubMedPMC
- 6. Asami K, Chae D. Influencing factors on health-related quality of life among Japanese middle-aged marriaged-based immigrant women in South Korea: A cross-sactional study. Journal of Korean Academy of Community Health Nursing. 2022;33(2):188–195. https://doi.org/10.12799/jkachn.2022.33.2.188Article
- 7. Mata J, Thompson RJ, Jaeggi SM, Buschkuehl M, Jonides J, Gotlib IH. Walk on the bright side: Physical activity and affect in major depressive disorder. Journal of Abnormal Psychology. 2012;121(2):297–308. https://doi.org/10.1037/a0023533ArticlePubMed
- 8. Liao Y, Shonkoff ET, Dunton GF. The acute relationships between affect, physical feeling states, and physical activity in daily life: A review of current evidence. Frontiers in Psychology. 2015;6:1975. https://doi.org/10.3389/fpsyg.2015.01975ArticlePubMedPMC
- 9. Niermann CYN, Herrmann C, von Haaren B, van Kann D, Woll A. Affect and subsequent physical activity: An ambulatory assessment study examining the affect-activity association in a real-life context. Frontiers in Psychology. 2016;7:677. https://doi.org/10.3389/fpsyg.2016.00677ArticlePubMedPMC
- 10. Flavián C, Ibáñez-Sánchez S, Orús C. Impacts of technological embodiment through virtual reality on potential guests’ emotions and engagement. Journal of Hospitality Marketing & Management. 2021;30(1):1–20. https://doi.org/10.1080/19368623.2020.1770146Article
- 11. Brimelow RE, Dawe B, Dissanayaka N. Preliminary research: Virtual reality in residential aged care to reduce apathy and improve mood. Cyberpsychology, Behavior, and Social Networking. 2020;23(3):165–170. https://doi.org/10.1089/cyber.2019.0286ArticlePubMed
- 12. Heyse J, Torres Vega M, De Jonge T, De Backere F, De Turck F. A personalised emotion-based model for relaxation in virtual reality. Applied Sciences. 2020;10(17):6124. https://doi.org/10.3390/app10176124Article
- 13. Schutte NS, Stilinović EJ. Facilitating empathy through virtual reality. Motivation and Emotion. 2017;41:708–712. https://doi.org/10.1007/s11031-017-9641-7Article
- 14. Yeo NL, White MP, Alcock I, Garside R, Dean SG, Smalley AJ, et al. What is the best way of delivering virtual nature for improving mood? An experimental comparison of high definition TV, 360 video, and computer generated virtual reality. Journal of Environmental Psychology. 2020;72:101500. https://doi.org/10.1016/j.jenvp.2020.101500ArticlePubMedPMC
- 15. Miller KJ, Adair BS, Pearce AJ, Said CM, Ozanne E, Morris MM. Effectiveness and feasibility of virtual reality and gaming system use at home by older adults for enabling physical activity to improve health-related domains: A systematic review. Age and Ageing. 2014;43(2):188–195. https://doi.org/10.1093/ageing/aft194ArticlePubMed
- 16. Song H, Peng W, Lee KM. Promoting exercise self-efficacy with an exergame. Journal of Health Communication. 2011;16(2):148–162. https://doi.org/10.1080/10810730.2010.535107ArticlePubMed
- 17. Alshaer A, O’Hare D, Archambault P, Shirley M, Regenbrecht H. How to observe users’ movements in virtual environments: Viewpoint control in a power wheelchair simulator. Human Factors. 2020;62(4):656–670. https://doi.org/10.1177/0018720819853682ArticlePubMed
- 18. Benzina N, Morgiève M, Euvrard M, Dos Santos JFA, Pelissolo A, Mallet L. Personalised 360° video exposure therapy for the treatment of obsessive-compulsive disorder: A single case study. French Journal of Psychiatry. 2020;1:31–38. https://doi.org/10.1016/j.fjpsy.2020.02.004Article
- 19. Dermody G, Whitehead L, Wilson G, Glass C. The role of virtual reality in improving health outcomes for community-dwelling older adults: Systematic review. Journal of Medical Internet Research. 2020;22(6):e17331. https://doi.org/10.2196/17331ArticlePubMedPMC
- 20. Lee N, Choi W, Lee S. Development of an 360-degree virtual reality video-based immersive cycle training system for physical enhancement in older adults: A feasibility study : Development of immersive virtual cycle for older adults. BMC Geriatrics. 2021;21(1):325. https://doi.org/10.1186/s12877-021-02263-1ArticlePubMedPMC
- 21. Teresi JA, Yu X, Stewart AL, Hays RD. Guidelines for designing and evaluating feasibility pilot studies. Medical Care. 2022;60(1):95–103. https://doi.org/10.1097/MLR.0000000000001664ArticlePubMedPMC
- 22. Li J, Hodgson N, Lyons MM, Chen KC, Yu F, Gooneratne NS. A personalized behavioral intervention implementing mHealth technologies for older adults: A pilot feasibility study. Geriatric Nursing. 2020;41(3):313–319. https://doi.org/10.1016/j.gerinurse.2019.11.011ArticlePubMedPMC
- 23. Sporrel K, Wang S, Ettema DDF, Nibbeling N, Krose BJA, Deutekom M, de Boer RDD, Simons M. Just-in-time prompts for running, walking, and performing strength exercises in the built environment: 4-week randomized feasibility study. JMIR Formative Research. 2022;6(8):e35268. https://doi.org/10.2196/35268ArticlePubMedPMC
- 24. Kandola A, Ashdown-Franks G, Hendrikse J, Sabiston CM, Stubbs B. Physical activity and depression: Towards understanding the antidepressant mechanisms of physical activity. Neuroscience & Biobehavioral Reviews. 2019;107:525–539. https://doi.org/10.1016/j.neubiorev.2019.09.040ArticlePubMed
- 25. Rajati F, Sadeghi M, Feizi A, Sharifirad G, Hasandokht T, Mostafavi F. Self-efficacy strategies to improve exercise in patients with heart failure: A systematic review. ARYA Atherosclerosis. 2014;10(6):319.PubMedPMC
- 26. Bandura A, Adams NE. Analysis of self-efficacy theory of behavioral change. Cognitive Therrapy and Research. 1977;1(4):287–310. https://doi.org/10.1007/BF01663995Article
- 27. Glanz K, Rimer BK, Viswanath K. Health behavior: Theory, research, and practice. 5th ed. San Francisco, CA: John Wiley & Sons; 2015. 485 p.
- 28. Polit DF, Beck CT. Nursing research: Generating and assessing evidence for nursing practice. 10th ed. Philadelphia: Wolters Kluwer Health; 2017. 814 p.
- 29. Clark L, Watson D. The Japanese Positive and Negative Affect Schedule: Factor-based scales for the assessment of mood. University of Iowa. 1989 (Unpublished).
- 30. Oka K. Stages of change for exercise behavior and self-efficacy for exercise among middle-aged adults. Nihon Koshu Eisei Zasshi. 2003;50(3):208–215. https://doi.org/10.11236/jph.50.3_208ArticlePubMed
- 31. Goulet-Pelletier JC, Cousineau D. A review of effect sizes and their confidence intervals, Part I: The Cohen’sd family. The Quantitative Methods for Psychology. 2018;14(4):242–265. http://doi.org/10.20982/tqmp.14.4.p242Article
- 32. Elo S, Kyngäs H. The qualitative content analysis process. Journal of Advanced Nursing. 2008;62(1):107–115. https://doi.org/10.1111/j.1365-2648.2007.04569.xArticlePubMed
- 33. Benham JL, Booth JE, Friedenreich CM, Rabi DM, Sigal RJ. Comparative success of recruitment strategies for an exercise intervention trial among women with polycystic ovary syndrome: Observational study. Journal of Medical Internet Research. 2021;23(3):e25208. https://doi.org/10.2196/25208ArticlePubMedPMC
- 34. Foster CE, Brennan G, Matthews A, McAdam C, Fitzaimons C, Mutrie N. Recruiting participants to walking intervention studies: A systematic review. The International Journal of Behavioral Nutrition and Physical Activity. 2011;8(1):1–28. https://doi.org/10.1186/1479-5868-8-137ArticlePubMedPMC
- 35. Gilliss CL, Lee KA, Gutierrez Y, Taylor D, Beyene Y, Neuhaus J, Murrell N. Recruitment and retention of healthy minority women into community-based longitudinal research. Journal of Women’s Health & Gender-Based Medicine. 2001;10(1):77–85. https://doi.org/10.1089/152460901750067142ArticlePubMed
- 36. Valente TW, Pumpuang P. Identifying opinion leaders to promote behavior change. Health Education & Behavior. 2007;34(6):881–896. https://doi.org/10.1177/1090198106297855ArticlePubMed
- 37. Nyenhuis SM, Balbim GM, Ma J, Marquez DX, Wilbur J, Sharp LK, Kitsiou S. A walking intervention supplemented with mobile health technology in low-active urban African American women with asthma: Proof-of-concept study. JMIR Formative Research. 2020;4(3):e13900. https://doi.org/10.2196/13900ArticlePubMedPMC
- 38. Jo A, Coronel BD, Coakes CE, Mainous Ⅲ AG. Is there a benefit to patients using wearable devices such as Fitbit or health apps on mobiles? A systematic review. American Journal of Medicine. 2019;132(12):1394–1400. e1. https://doi.org/10.1016/j.amjmed.2019.06.018ArticlePubMed
- 39. Browning MHEM, Mimnaugh KJ, van Riper CJ, Laurent HK, LaValle SM. Can simulated nature support mental health? Comparing short, single-doses of 360-degree nature videos in virtual reality with the outdoors. Frontiers in Psychology. 2020;10:2667. https://doi.org/10.3389/fpsyg.2019.02667ArticlePubMedPMC
- 40. Seiluri T, Lahti J, Rahkonen O, Lahelma E, Lallukka T. Changes in occupational class differences in leisure-time physical activity: A follow-up study. International Journal of Behavioral Nutrition and Physical Activity. 2011;8(1):1–8. https://doi.org/10.1186/1479-5868-8-14ArticlePubMedPMC
- 41. Baumeister H, Reichler L, Munzinger M, Lin J. The impact of guidance on Internet-based mental health interventions — A systematic review. Internet Interventions. 2014;1(4):205–215. https://doi.org/10.1016/j.invent.2014.08.003Article
- 42. Michie S, Yardley L, West R, Patric K, Greaves F. Developing and evaluating digital interventions to promote behavior change in health and health care: Recommendations resulting from an international workshop. Journal of Medical Internet Research. 2017;19(6):e232. https://doi.org/10.2196/jmir.7126ArticlePubMedPMC
- 43. Brickwood KJ, Watson G, O'Brien J, Williams AD. Consumer-based wearable activity trackers increase physical activity participation: Systematic review and meta-analysis. JMIR mHealth and uHealth. 2019;7(4):e11819. https://doi.org/10.2196/11819ArticlePubMedPMC
- 44. Gal R, May AM, van Overmeeren EJ, Simons M, Monninkhof EM. The effect of physical activity interventions comprising wearables and smartphone applications on physical activity: a systematic review and meta-analysis. Sports Medicine-Open. 2018;4(1):1–15. https://doi.org/10.1186/s40798-018-0157-9ArticlePubMedPMC
- 45. Laranjo L, Ding D, Heleno B, Kocaballi B, Quiroz JC, Tong HL, et al. Do smartphone applications and activity trackers increase physical activity in adults? Systematic review, meta-analysis and metaregression. British Journal of Sports Medicine. 2021;55(8):422–32. http://dx.doi.org/10.1136/bjsports-2020-102892ArticlePubMed
- 46. El Masri A, Kolt GS, George ES. Feasibility and acceptability of a culturally tailored physical activity intervention for Arab-Australian women. BMC Womens Health. 2021;21(1):1–14. https://doi.org/10.1186/s12905-021-01250-3ArticlePubMedPMC
- 47. Knapp TR. Why is the one-group pretest–posttest design still used? Clinical Nursing Research. 2016;25(5):467–472. https://doi.org/10.1177/1054773816666280ArticlePubMedPDF
- 48. Shiffman S, Stone AA, Hufford MR. Ecological momentary assessment. Annual Review of Clinical Psychology. 2008;4:1–32. https://doi.org/10.1146/annurev.clinpsy.3.022806.091415ArticlePubMed
 PubReader
PubReader ePub Link
ePub Link Cite
Cite